
Current theories of the obesity epidemic are inadequate. None of them hold up to closer scrutiny, and none can explain all of the mysteries mentioned in Part I. But these mysteries are real, puzzling data about the obesity epidemic.
You’re probably familiar with several theories of the obesity epidemic, but there is strong evidence against all of them. In this section, we focus on the case against a couple of the most popular theories.
2.1 Calories In, Calories Out
A popular theory of obesity is that it’s simply a question of calories in versus calories out (CICO). You eat a certain number of calories every day, and you expend some number of calories based on your metabolic needs and physical activity. If you eat more calories than you expend, you store the excess as fat and gain weight, and if you expend more than you eat, you burn fat and lose weight.
This perspective assumes that the body stores every extra calorie you eat as body fat, and that it doesn’t have any tools for using more or less energy as the need arises. But this isn’t the case. Your body has the ability to regulate things like its temperature, and it has similar tools to regulate body fatness. When we look closely, it turns out that “calories in, calories out” doesn’t match the actual facts of consumption and weight gain.
“This model seems to exist mostly to make lean people feel smug,” writes Stephen Guyenet, “since it attributes their leanness entirely to wise voluntary decisions and a strong character. I think at this point, few people in the research world believe the CICO model.”
It’s not that calories don’t matter at all. People who are on a starvation diet of 400 calories per day will lose weight, and as we will see in this section, people who eat hundreds of calories more than they need will usually gain weight. The problem is that this ignores how the body accounts for the calories coming in and going out. If you don’t eat enough, your body finds ways to burn fewer calories. If you eat too much, your body doesn’t store all of the excess as fat, and compensates by making you less hungry later on. Calories are involved in the math but it’s not as simple as “weight gain = calories in – calories out”.
[Edit: We’ve added an interlude clarifying this section on CICO in response to reader questions and objections. If you have objections to anything below, read the interlude here because we probably address it!]
2.1.1 Common Sense
First, we want to present some common-sense arguments for why diet and exercise alone don’t explain modern levels of obesity.
Everyone “knows” that diet and exercise are the solution to obesity. Despite this, rates of obesity continue to increase, even with all the medical advice pointing to diet and lifestyle interventions, and a $200 billion global industry devoted to helping people implement these interventions. It’s not that no one is listening. People are exercising more today than they were 10 or even 20 years ago. Contrary to stereotypes, more than 50% of Americans meet the HHS guidelines for aerobic exercise. But obesity is still on the rise.
It’s true that people eat more calories today than they did in the 1960s and 70s, but the difference is quite small. Sources have a surprisingly hard time agreeing on just how much more we eat than our grandparents did, but all of them agree that it’s not much. Pew says calorie intake in the US increased from 2,025 calories per day in 1970 to about 2,481 calories per day in 2010. The USDA Economic Research Service estimates that calorie intake in the US increased from 2,016 calories per day in 1970 to about 2,390 calories per day in 2014. Neither of these are jaw-dropping increases.
If we go back further, the story actually becomes even more interesting. Based on estimates from nutrient availability data, Americans actually ate more calories in 1909 than they did in 1960.
Finally, there are many medical conditions that cause obesity. For example, Prader-Willi Syndrome, a genetic disorder characterized by intense hunger and resulting obesity, hypothyroidism, an endocrine disorder where people experience loss of appetite yet still gain 5-10 pounds, and lesions to the hypothalamus, which often lead to intense weight gain, sometimes accompanied by great hunger but many times not.
2.1.2 Scientific Evidence
In addition to these common-sense objections, decades of research suggests that diet and exercise are not to blame for rising rates of obesity.
Studies of controlled overfeeding — you take a group of people and get them to eat way more than they normally would — reliably find two things. First, a person at a healthy weight has to eat huge amounts of calories to gain even a couple pounds. Second, after the overfeeding stops, people go right back to the weight they were before the experiment.
The great-grandaddy of these studies is the Vermont prison experiment, published in 1971. Researchers recruited inmates from the Vermont State Prison, all at a healthy weight, and assigned some of them to eat enormous amounts of food every day for a little over three months. How big were these meals? The original paper doesn’t say, but later reports state that some of the prisoners were eating 10,000 calories per day.
On this olympian diet, the prisoners did gain considerable weight, on average 35.7 lbs (16.2 kg). But following the overfeeding section of the study, the prisoners all rapidly lost weight without any additional effort, and after 10 weeks, all of them returned to within a couple pounds of their original weight. One prisoner actually ended up about 5 lbs (2.3 kg) lighter than before the experiment began!
Inspired by this, in 1972, George Bray decided to conduct a similar experiment on himself. He was interested in conducting overfeeding studies, and reasoned that if he was going to inflict this on others, he should be willing to undergo the procedure himself. First he tried to double each of his meals, but found that he wasn’t able to gain any weight — he simply couldn’t fit two sandwiches in his stomach at every sitting.
He switched to energy-dense foods, especially milkshakes and ice cream, and started eating an estimated 10,000 calories per day. Soon he began to put on weight, and gained about 22 lbs (10 kg) over 10 weeks. He decided this was enough and returned to his normal diet. Six weeks later, he was back at his original weight, without any particular effort.
In both cases, you’ll notice that even when eating truly stupendous amounts of food, it actually takes more time to gain weight than it does to lose it. Many similar studies have been conducted and all of them find basically the same thing — check out this recent review article of 25 studies for more detail.
Overfeeding in controlled environments does make people gain weight. But they don’t gain enough weight to explain the obesity epidemic. If you eat 10,000 calories per day, you might be able to gain 20 or 30 pounds, but most Americans aren’t eating 10,000 calories per day.
We can compare these numbers to the increases in average calories per day we reviewed earlier. Sure, consumption in the US went from 2,025 calories per day in 1970 to 2,481 calories per day in 2010, a difference of 456 calories. But consider Poehlman et al. (1986), where researchers fed a group of 12 men 1,000 extra calories a day for 22 days. On average the men gained about 5 lbs (2.2 kg), but some of them actually lost weight instead.
And it’s not as though these participants are eating 1,000 extra calories of celery and carrots. In one study, the extra calories came from “sherbet, fruit juices, margarine, corn oil, and cookies”. But the content doesn’t seem to matter very much. Another study compared overfeeding with carbohydrates (mostly starch and sugar) and overfeeding with fat (mostly dairy fat like cream and butter). The two groups got their extra calories from different sources, but they were overfed by the same amount. After two weeks, both groups gained the same amount of fat, 3.3 lbs on average. A similar study overfed volunteers by 1,194 calories on either a high-carb or a high-fat diet for 21 days. Both groups gained only about 2 lbs of fat.
The fact that many of these are twin studies provides even more evidence against CICO. In groups of twins that are all overfed by the same amount, there is substantial variation between the different participants in general. Some people gain a lot of weight, others gain almost none. But each person gains (or loses!) about the same amount of weight as their twin. In some cases these correlations can be substantial, as high as r = 0.90. This strongly suggests that genetics plays a large role in determining how the body responds to overfeeding.
The story with exercise is the same as with overeating — it makes a difference, but not much. One randomized controlled trial assigned overweight men and women to different amounts of exercise. More exercise did lead to more body fat loss, but even in the group exercising the most — equivalent to 20 miles (32.0 km) of jogging every week for eight months — people only lost about 7 lbs.
You might think that hunter-gatherers have a more active lifestyle than we do, but this isn’t always true. The Kitavans examined in 1990 by Staffan Lindeberg were only slightly more active than westerners, had more food than they knew what to do with, and yet were never obese. “Many Westerners have a level of physical activity that is well within the range of the Kitava population,” he wrote. “Hence, physical activity does not seem to explain most of the differences in disease pattern between Kitava and the Western world.”
A recent meta-analysis of 36 studies compared the effects of interval training exercise with more traditional moderate-intensity continuous training. The authors call interval training “the magic bullet for fat loss” (this is literally in the title) and trumpet that it provides 28.5% greater reductions in total absolute fat mass than moderate exercise. But what they don’t tell you is that this is a difference between a loss of about 3 lbs and about 4 lbs, for an exercise program running 12 weeks long. Needless to say, this difference isn’t very impressive. Other meta-analyses find similar results: “neither short-term HIIT/SIT nor MICT produced clinically meaningful reductions in body fat.”
Maybe diet and exercise together are worth more than the sum of their parts? Sadly this doesn’t seem to be the case either. If anything, when combined they are worth less than the sum of their parts. One meta-analysis comparing interventions based on diet, exercise, and diet plus exercise found that people lost about 23.5 lbs (10.7 kg) on diets, 6.4 lbs (2.9 kg) on an exercise regime, and 24.2 lbs (11.0 kg) on diet plus exercise. After a year, diet plus exercise was down to 18.9 lbs (8.6 kg). Other meta-analyses are more tempered, for example, finding a loss of about 3.6 lbs (1.6 kg) after two years of diet plus exercise interventions. Again this is more weight loss than zero, but it clearly rules out diet plus exercise as an explanation for the obesity epidemic. People in 1950 were a lot leaner than they are now, but it’s not because they ate less and exercised more.
2.2 Good Calories and Bad Calories
Ok, calories themselves may not be the villain here. But maybe it’s not that we’re eating more than we used to — maybe it’s that we’re eating differently. Maybe one particular macronutrient or source of calories is to blame.
2.2.1 Dietary Fat
Dietary fat seems like a possible culprit. After all, fat makes you fat, right? Turns out it’s not so simple.
To begin with, fat consumption has actually fallen over the past few decades, while obesity has skyrocketed. This isn’t consistent with an explanation where dietary fat leads to obesity.
Plenty of cultures eat extremely high-fat diets and remain very lean indeed. You’ll remember that the Maasai diet is about 3000 calories per day, and 66% of that is from fat. But the Maasai don’t suffer from obesity. In fact, Kalahari Bushmen love fat and apparently wax poetic about it.
Clinical results agree: dietary fat doesn’t have much of an impact on long-term weight. Putting people on a low-fat diet reduces their weight in the short term, but in trials lasting for longer than one year, they tend to return to normal. When they are directly compared, low-fat and high-fat diets have about the same impact on weight loss.
This is a little difficult to square with animal studies that find that a high-fat diet reliably leads to obesity in monkeys, dogs, pigs, hamsters, squirrels, rats, and mice. It could just be that humans are not monkeys, dogs, pigs, hamsters, squirrels, rats, or mice, and that while dietary fat has an adverse effect on these species, it doesn’t do much to us. Some of the hamster studies, for example, induced obesity simply by giving the hamsters extra sunflower seeds, a phenomenon not observed in humans. Pigs, in particular, will become obese even on low-fat diets when given the opportunity.
We even see differences within a specific kind of animal. The same high-fat diet will make one species of hamster (Syrian hamsters) obese and leave another species of hamster (golden hamsters) merely chubby. If the findings can’t generalize between different species of hamsters, we shouldn’t expect them to generalize to humans.
It could also be that dietary fat leads to obesity in mammals held in captivity, possibly due to factors like stress. Metabolic ward studies restrict your movement, but it’s not exactly like living your whole life in a laboratory cage. And it’s worth noting that about 10–15% of macaque and rhesus monkeys in captivity become obese when they reach middle age, despite the fact that they are fed a relatively low-fat (10% of energy) diet.
In any case, it’s hard to square a fat-based explanation for the obesity epidemic with the fact that fat consumption hasn’t increased in step with the rise of obesity and the fact that low-fat diets don’t lead to much weight loss.
2.2.2 Carbohydrates
Ok, maybe fat doesn’t make you fat. How about carbohydrates? All this bread can’t be good for us.
This theory is dead on the starting line, though, because as obesity has gone up, consumption of carbohydrates has gone down (see figure).
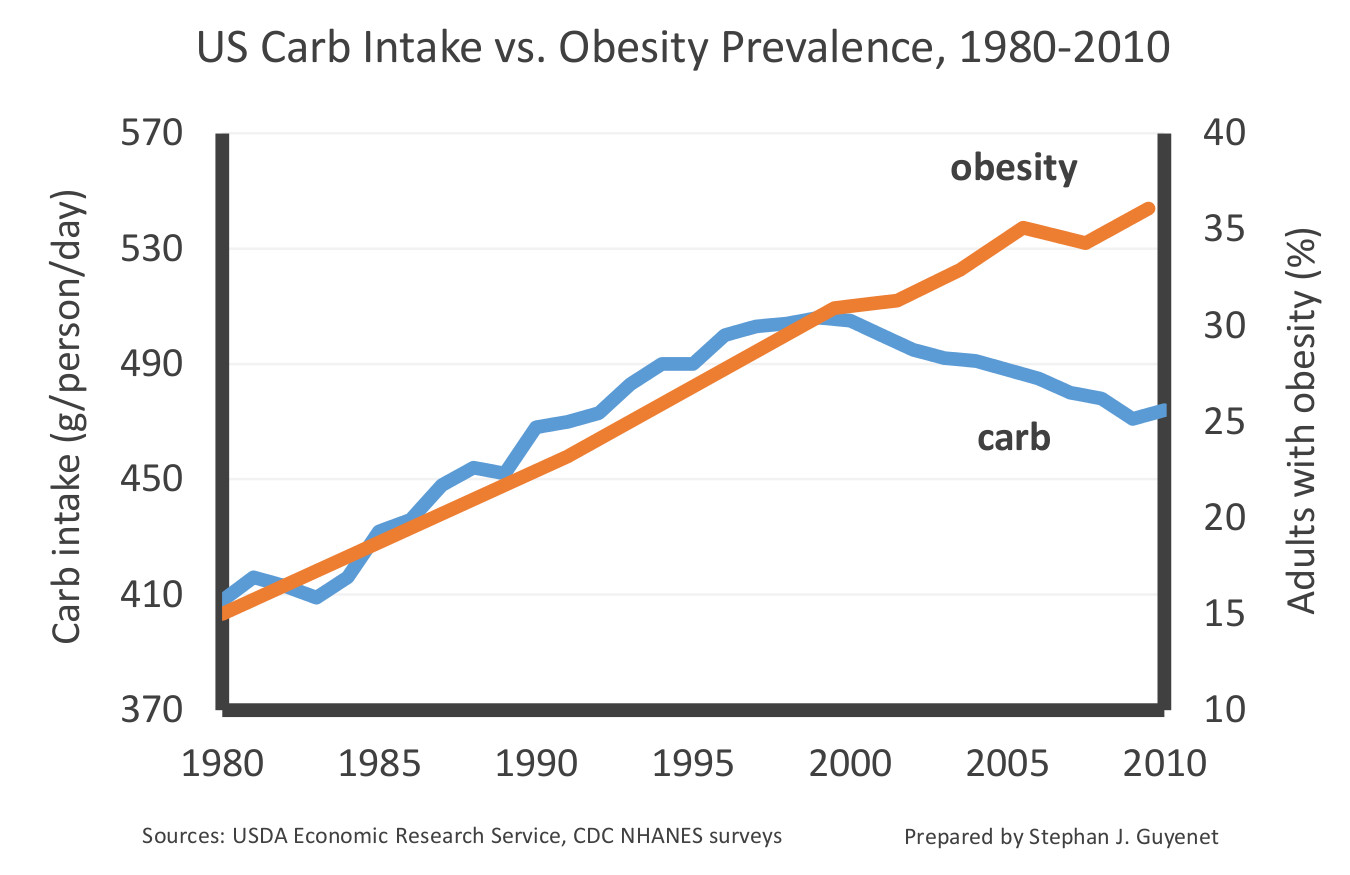
This is enough to make it clear that carbohydrate consumption isn’t driving the obesity epidemic, but we can take a slightly closer look anyways, just to be sure.
Eating lots of carbs can actually make you lose weight. High-carbohydrate diets cause weight loss, even when not restricting calories. A study from 2003 examined low-fat diets in 16 overweight people. Naturally, this low-fat diet was high in carbohydrates. When patients started the low-fat diet and were told to eat as much as they wanted, they actually ate 291 calories less per day.
But their carbohydrate intake increased, from 253 grams per day to 318 grams per day. On this diet they lost 8 lbs (3.8 kg) on average over a 12-week period. In the DIETFITS randomized controlled trial, 609 people fed a whole-food, high-carbohydrate diet lost 12 pounds (5.3 kg) over one year, not significantly different from the 13 pounds (6.0 kg) of weight lost on a whole-food low-carbohydrate diet. The high-carbohydrate diet also supplied about 1.5 times as much sugar as the low-carbohydrate diet.
The residents of Kitava, mentioned earlier, have a diet of starchy roots and tubers. Almost 70% of their calories come from carbohydrates, but they don’t suffer from obesity, diabetes, or heart disease.
(Lindeberg also says: “The long primate history of fruit eating, the high activity of human salivary amylase for effcient starch digestion, and some other features of human mouth physiology … suggest that humans are well prepared for a high carbohydrate intake from non-grain food sources. … in contrast to most other animals including non-human primates, humans have an exceptional capacity to produce salivary amylase in order to begin hydrolysis of starch in the mouth.”)
In general, cultures with very high intakes of carbohydrate tend to be lean. Most agricultural societies around the world have a diet that is high in carbohydrates and low in fat. Agricultural societies are different from industrialized ones in many ways, of course. But even in those agricultural cultures with abundant food, people are typically lean, with low rates of diabetes and cardiovascular disease.
This is true even if the carbohydrate is white rice. In Japan, white rice is a primary staple food (p. 338), and has been for a long time. About 62% of the Japanese diet is carbohydrates, and most of this is white rice. Despite this, Japanese rates of obesity have been, and continue to be, the lowest of any industrialized nation.
In fact, people who move from Japan to the US and begin eating less white rice become much heavier. This suggests that the difference isn’t simply genetic. These immigrants do end up eating a diet much higher in fat — but of course, from the previous section, we’ve seen that fat can’t be responsible for this change.
Nor is it likely to be some other carbohydrate staple. Wheat consumption, for example, has been falling for a century. People in the US ate almost twice as much wheat (primarily in the form of bread) in the 1880’s than they do today. If wheat were responsible, people would have been massively obese during reconstruction and entirely lean today. Obviously that is not what we observe.
If the historical data isn’t enough for you, there are entire reviews devoted to the health impacts of wheat, pretty conclusively showing that it isn’t a cause of obesity.
2.2.3 Sugar
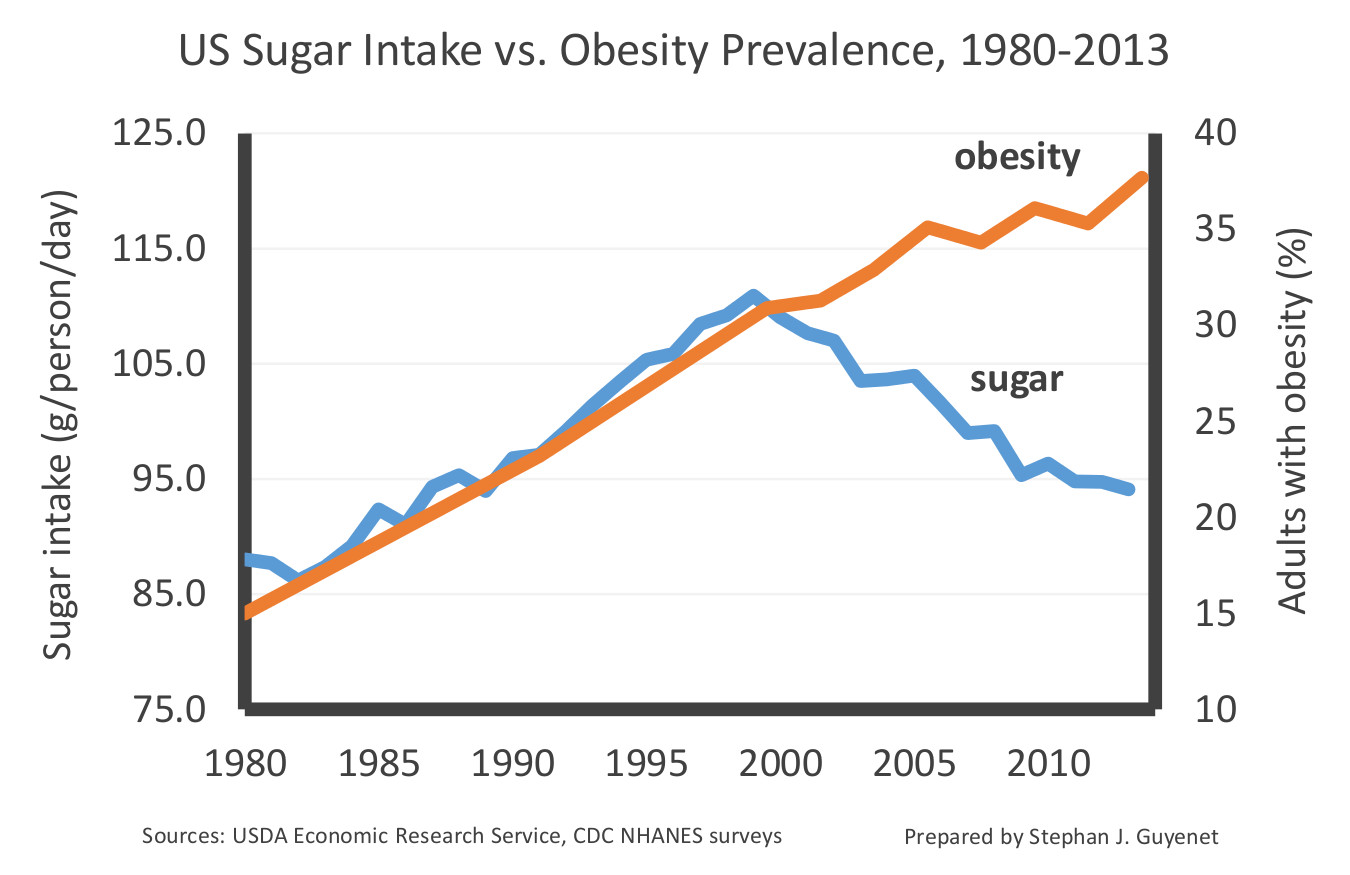
Everyone knows that added sugar is the real villain, right? Wrong again.
Sugar consumption has been declining for 20 years in the US, while obesity and diabetes rates have increased. The sugar data in the figure below includes all added sugars such as honey, table sugar, and high-fructose corn syrup, but doesn’t include sugars naturally occurring in fruits and vegetables.
We see something similar in what has been called The Australian Paradox, where obesity in Australia nearly tripled between 1980-2003, while sugar consumption dropped 23%.
Multiple lines of evidence confirm that sugar consumption is falling worldwide. In the US, consumption of sugary beverages dropped between 1999 and 2010. We see the same trend in longitudinal studies of a particular cohort tracked from 1991 to 2008. It’s not that consumers can’t find the sugar they crave, of course — there have been no major changes in the availability of sugary foods.
We see that public health efforts to reduce sugar consumption have worked. In fact, they’ve worked very well. But they don’t seem to have made any difference to the obesity epidemic.
Tightly-controlled metabolic ward studies also show that the sugar content of a diet doesn’t matter much. One study of 17 men compared a 25 percent sugar, high-carbohydrate diet to a 2 percent sugar, very-low-carbohydrate (ketogenic) diet of equal calories. After four weeks, they found that the high-carbohydrate diet caused slightly more body fat loss than the very-low-carbohydrate (ketogenic) diet, despite the fact that the two diets differed more than tenfold in sugar content. We see similar results in mice and in rats: “Animals fed a low-fat, high-sucrose (LH) diet were actually leaner than animals fed a high-complex-carbohydrate diet.”
We can further cite the fact that many cultures, such as the Hadza of Tanzania, the Mbuti of the Congo, and the Kuna of Panama all eat diets relatively high in sugar (sometimes as high at 80%), and yet none of these cultures have noticeable rates of obesity, diabetes, cardiovascular disease, etc.
2.3 Diet in General
Over the past 40 years, there hasn’t been much of a change in where people get their calories from. Americans get about 50% of their calories from carbohydrates, 30% from fat, and 20% from protein, and they have for years. At the same time obesity continues to go up and up. Comparing these two trends, it’s hard to imagine that macronutrients have anything to do with the obesity epidemic.
You’ll recall that Mystery 8 is that all diets work about equally well. It doesn’t matter which diet you choose — you lose about the same number of pounds regardless.
All diets work. The problem is that none of them work very well. Stick to just about any diet for a couple weeks and you will probably lose about 10 pounds. This is ok, but it isn’t much comfort for someone who is 40 lbs overweight. And it isn’t commensurate with the size of the obesity epidemic.
Systematic comparison of weight-loss diets with different compositions of fat, protein, and carbohydrates finds that across many different reduced-calorie diets, people lose about 13.2 lbs (6 kg) over six months, and that in all cases people began to gain weight back after 12 months. It’s not just weight loss, either. Satiety, hunger, satisfaction with the diet, and adherence to the protocol is similar for all diets.
There are too many diets to review in full, of course, but we see the same pattern in every diet that has been extensively studied. Let’s look at just a few.
2.3.1 Ketogenic Diet
We’ve already mentioned a few ketogenic diets, and as we’ve seen, they don’t work much better than other diets do.
There is one meta-analysis of ketogenic diet studies, comparing very-low-carbohydrate ketogenic diets to low fat diets in overweight and obese adults. Across thirteen randomized controlled trials, ketogenic diets only caused 2 pounds (0.9 kg) more weight loss than the traditional low-fat diets after 12 months.
2.3.2 Low-Glycemic Diet
Study after study finds that low-glycemic diets don’t work for weight loss.
One study from 2007 randomly assigned 203 women to either a high-glycemic or low-glycemic diet. The difference in glycemic index was considerable, with the high-glycemic diet having an index twice as high as the low-glycemic diet. The groups consumed the same amount of calories and reported similar levels of hunger.
Despite this, there was no difference between the groups. After two months the LGI group had lost 1.6 lbs (0.72 kg) and the HGI group had lost 0.7 lbs (0.31 kg), but this difference wasn’t sustained. After 18 months on the diet, the LGI group had lost 0.9 lbs (0.41) kg and the HGI group had lost 0.6 lbs (0.26 kg), and this difference was statistically indistinguishable (p = .93). Large differences in glycemic index have no meaningful long-term (or even short-term) effect on calorie consumption or body weight.
Another 18-month randomized trial compared a low-glycemic load (40% carbohydrate and 35% fat) vs low-fat (55% carbohydrate and 20% fat) diet in 73 obese young adults in the Boston, Massachussets area. In both diets, participants were largely eating whole foods; vegetables, beans, and fruit were major components of both diets. In both diets, people were allowed to eat as much as they wanted.
Both groups reported similar levels of hunger and consumed similar amounts of calories. The two diets were rated equally easy to stick to and equally tasty. Both groups lost about 4-5 lbs after 6 months. But both groups started to gain weight back soon after. In fact, the trajectory of weight loss is so identical, we simply have to show you the graph:

Note the p-value of 0.99, which indicates that the two trajectories are about as statistically indistinguishable as is mathematically possible.
We find this in study after study. Meta-analysis also finds that low-glycemic diets don’t do any better than other diets when it comes to weight loss. When the reviewers pick out the studies that show the best performance for low-glycemic diets, they still find a difference of only 4 lbs (1.8 kg). If that’s a success, we have to wonder what failure would look like.
2.3.3 Future Dietary Explanations
Eating fewer calories will lead most people to lose a couple pounds, and it doesn’t really matter what calories they restrict. Cutting back on fat works about as well as cutting back on carbs. In both cases, a couple pounds isn’t enough to explain the obesity epidemic.
Over the past 50 years, medical science has looked at diet from practically every angle. But none of these diet-based explanations have gone anywhere. People are still getting fatter. They got fatter over the last decade. And they got fatter over the decade before that. And the one before that. Every country in the world is growing more obese. And the trend has never once been reversed.
You could certainly cook up another diet-based explanation. But there’s no reason to expect that this explanation would do any better than any of the others.
It’s time to start looking for explanations outside the world of calories, macronutrients, and exercise. At this point, we should assume that the obesity epidemic isn’t caused by our diet.
Could it be a lifestyle difference? Possibly, but signs point against it. Smoking is more prevalent in Japan than among Japanese-Americans, yet Japanese-Americans have much higher rates of hypertension. Similarly, many hunter-gatherers are heavy smokers, including the Kitavans (76% of men and 80% of women) and the Bushmen of South Africa, but these societies have no sign of heart disease.
2.5 Lipostat
There is one theory of obesity which is almost entirely satisfying, based around the body’s ability to regulate its adiposity.
A house has a thermostat. The owner of the house sets the temperature to 72 degrees F. The thermostat detects the temperature of the house and takes action to drive the temperature to the set point of 72°F. If the house is too cold, the thermostat will turn on the furnace. If the house is too warm, the thermostat will turn on the air conditioning.
The human body has a lipostat (from the Greek lipos, meaning fat). Evolution and environmental factors set body fatness to some range — perhaps a BMI of around 23. The lipostat detects how much fat is stored and takes action to drive body fatness to the set point of a BMI of 23. If your body is too thin, the lipostat will drive you to eat more, exercise less, sleep more, and store more of what you eat as fat. If your body is too fat, the lipostat will turn on the air conditioning. Just kidding, the lipostat will drive you to eat less, move and fidget more, and store less of the food you eat as fat.
According to this theory, people become obese because something has gone wrong with the lipostat. If the owner of a house sets the thermostat to 120°F, the house will quickly become too hot, and it will stay that way until the set point is changed or the furnace explodes. Something similar is happening in obesity. The set point has been moved from a healthy and natural level of adiposity (BMI of about 23) to an unusually high level (BMI 30+), and all the regulatory systems of the body are working in concert to push adiposity to that level and keep it there.
The lipostat model is supported by more than a hundred years of evidence. By the 1970s, Dr. Michel Cabanac and collaborators were publishing papers in the journal Nature on what they called the “ponderostat” (pondero = weight). This was later revised to the adipostat (adipo = fat), and eventually, as we call it here, the lipostat.
Modern neuroscience and medical review articles (those are three separate links) overwhelmingly support this homeostatic explanation. In animals and humans, brain damage to the implicated areas leads to overeating and eventual obesity. These systems are well-understood enough that by targeting certain neurons you can cure or cause obesity in mice. While we don’t approve of destroying neurons in human brains with hyperspecific chemical techniques, the few weight-loss drugs approved by the FDA largely act on the brain (hopefully without destroying any neurons).
The lipostat explains why diet and exercise work a little, why they don’t work well enough to reverse obesity, and why even people who lose weight on diets generally end up gaining that weight right back.
In a house where the thermostat has been set to 120°F, there are a lot of things we can do to lower the temperature. We can open all the doors and windows. We can open the icebox. We can order mountains of dry ice off of the internet. All of these things will lower the temperature of the house a little, but even with these measures, the house will still be hotter than the healthy temperature of 72ºF. The furnace will work double-time to push the temperature back up to 120ºF, if it’s not redlining already. And as soon as you relax any of your heat-dissipation measures, the temperature will go right back up to where it was before.
(We can also go down into the basement and hit the furnace with crowbars until it doesn’t work very well anymore. This is a pretty extreme solution and also, incidentally, why gastric bypass surgery works so great.)
When people intentionally overeat, as in the overfeeding studies we reviewed, they temporarily gain a little weight, but when they stop overeating, they quickly return to their original weight. When people intentionally undereat, as they do on a diet, they temporarily lose a little weight, but when they stop undereating they quickly return to their original weight. In fact, they usually return to near their original weight even if they keep undereating. The lipostat has a target weight and, when not actively opposed, it will push your body weight to that weight and do its best to keep it there.
There are many signals that the brain uses to measure how much fat the body is carrying. One of the most important is the hormone leptin, which is naturally produced by fat cells. Part of the action of the lipostat is making sure that leptin levels are kept within a desired range, which helps keep us at a desired weight.
Very rarely, people are born with a genetic mutation that makes it so their fat cells no longer produce leptin. The lipostat notices that it isn’t detecting any leptin, and assumes that the body has no fat stores at all, with predictable results. Usually these children are of normal birth weight, but from the first weeks of their lives, they are insatiably hungry. By age two, they weigh more than 50 pounds, and may be as high as 60% fat by weight. They have a truly incredible drive to eat:
. . . leptin-deficient children are nearly always hungry, and they almost always want to eat, even shortly after meals. Their appetite is so exaggerated that it’s almost impossible to put them on a diet: if their food is restricted, they find some way to eat, including retrieving stale morsels from the trash can and gnawing on fish sticks directly from the freezer. This is the desperation of starvation [. . . ] they become distressed if they’re out of sight of food, even briefly. If they don’t get food, they become combative, crying and demanding something to eat.
The lipostat account is extremely convincing. The only weakness in the theory is that it’s not clear what could cause the lipostat to be set to the wrong point. In leptin-deficient children, their body simply can’t detect that they are obese. But most people produce leptin just fine. What is it that throws this system so totally out of balance?
While the lipostat perspective does in a sense explain why people become obese (their lipostat is out of alignment), it’s not really a theory of the obesity epidemic, since it doesn’t explain why our lipostats began getting more and more out of balance around 1980.
Even advocates of the theory are perfectly willing to admit this. In The Hungry Brain, Stephen Guyenet writes:
Many researchers have tried to narrow down the mechanisms by which [diet] causes changes in the hypothalamus and obesity, and they have come up with a number of hypotheses with varying amounts of evidence to support them. Some researchers believe the low fiber content of the diet precipitates inflammation and obesity by its adverse effects on bacterial populations in the gut (the gut microbiota). Others propose that saturated fat is behind the effect, and unsaturated fats like olive oil are less fattening. Still others believe the harmful effects of overeating itself, including the inflammation caused by excess fat and sugar in the bloodstream and in cells, may affect the hypothalamus and gradually increase the set point. In the end, these mechanisms could all be working together to promote obesity. We don’t know all the details yet…
Guyenet favors a “food reward” explanation, where eating “highly rewarding food” causes a mild form of brain damage that turns up the set point of the lipostat. He’s even gone so far as to propose (as an April Fools joke) a collection of boring recipes called The Bland Food Cookbook.
You’ll notice that in all these theories, the factors that damage the lipostat are related to diet. But as we’ve just argued above, the persistent failure to find a solution in our diets strongly suggests that we should start looking elsewhere for the explanation.
2.6 What, Then?
We should start seriously considering other paradigms. If diet and exercise are out as explanations for the epidemic, what could possibly explain it? And what could possibly explain all of the other bizarre trends that we have observed?
[Next Time: A CHEMICAL HUNGER]

Nice, Some random thoughts while reading.
It would be pretty easy to make the case that evolution has shaped humans to accept a wide range of diets. Which also means people with different ancestry may have different adaptations. Lactose tolerance being an easy recent example. (Corollary, Be careful applying diet studies across human populations, and other animals more so.)
Carbs and weight lose; Don’t tell me I will lose weight by eating those gooey sugary spearmint candies I buy and love!
Waiting for part 3. I stumbled on a nice paper by Paula Baillie-Hamilton, the link should clearly go in the comments of that section.
LikeLike
You said we’re eating less fat, less sugar and less carbs, but then said the fat/carb/protein ratio has remained the same. So are we just eating less?
My feeling has long been that sugary+caffeinated drinks must be involved, and/or other ultra-high glycemic load food. Even if overall sugar has decreased, a banana is very different from a can of coke. You can have a meal’s worth of calories without any satiation, while the caffeine pumps up your digestion, and the glycemic spike does weird things to your body.
I don’t think anything you’ve written so far contradicts this ide?
LikeLike
I guess we’re eating more protein?
LikeLike
This is a great question, and something we’ve wondered about as well. The ratio has remained roughly the same — there’s certainly a small increase in protein consumption according to most sources. We may also be eating less over the past 10 years, eyeballing some charts it looks like overall consumption has been falling since about the year 2000.
Well, a few things come to mind. We haven’t seen much evidence that glycemic load matters, and there’s some evidence that it doesn’t. Sugary drinks existed well before 1970 so that makes them an unlikely culprit to us. And it doesn’t seem like this could explain the altitude effect. In terms of soda in particular, we know David B. Allison has done some work which is kind of mixed, but at least doesn’t find a strong effect of soda consumption, e.g.: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3929296/
LikeLike
Surely the quantity of sugary drinks available easily at once and at a low cost is vastly different over the timeframe you are looking at. In the study you link to, they only add 150 kCals per day to the kids diets, which is just one 12oz coke. Quick search shows a McDonald’s medium is 21oz and large is 32oz, so regularly people are getting doses of 68g – 104g of sugar in liquid form along with their food.
The “human food does something different to rats” observation seems to fit with some set of nutrients overloading the brain’s satiation detector. It might be sugar and salt at once in the case of sodas, or another pairing with fruit loops (which has 1/3 the sugar of coke but 3x the sodium per serving apparently).
Just anecdotally, in the process of figuring out what I can eat to allow consistent weight loss or at least maintenance, I now can tell the times when something throws me “off the wagon” and I start wanting to eat way more than I need, without satiation. It does feel like something dose dependent around sugary foods but I haven’t fully pinned down what foods / set of foods does that.
LikeLike
I think this article is a good explanation of how people commonly misunderstand the CICO model: https://sigmanutrition.com/cico/
I think you’re being a little hard on it here, but I do agree that some of its tenets that have leaked into the popular narrative are misleading and/or inaccurate.
LikeLike
Your counterargument to CICO seems quite weak.
In the common sense section, while you say “the difference is quite small”, note that the difference is *bigger* than the BMI difference for that time periods. People are eating 20% more calories between 1970 and 2010-14 and we would naively expect them to have 20% greater weight and hence 20% higher BMI. But BMIs have only increased by 10%. Maybe the extra exercise is helping?
On the other hand, people in 1960 ate the same as or less than people in 1900. But did they exercise less too? You only say exercise has been increasing recently, and I bet there was a lot more manual labor for jobs (farming and construction) and chores in 1909.
In the scientific evidence section, you provide a great example where CICO *is* likely to fail. Your digestive tract probably can’t take up most of the 4x normal calories in a 10k/day diet. However, in a 1.4x normal diet of only 1k extra calories a day, men gain a more reasonable 1 pound per 4.4k calories. The normal quoted number is 3.5k calories per pound. Although your other quoted study has 1 pound per 13k calories, which does give me pause…
I dislike that people treat CICO as mutually exclusive with other models and feel the need to debunk it. We can accept that eating more leads to weight gain but also accept that controlling your urges is hard. E.g. both CICO and Lipostat can be good models at the same time. Even if the whole obesity epidemic is “explained” by people eating more, I still found your first post riveting and excitedly anticipate your proposal for why it’s happening. Did weird chemicals break our lipostats?
LikeLiked by 1 person
I’m not sure we would naively expect 20% in one place to translate to 20% in another place, especially since BMI is a weird measure, but open to being convinced.
It doesn’t seem likely to be the result of exercise, since (for example) farm laborers and construction workers are more obese now than they were in the 1960s. Conversely, many people in 1909 had cushy desk jobs and almost none of them were obese.
CICO is kind of an uncomfortable mix of hard-to-separate hypotheses, so we appreciate your pushing back on this. Here’s an effort to try to separate some of this:
One sub-hypothesis is that overeating by the same amount always leads to the same amount of weight gain — for example, the 3.5k calories per pound you mention. The controlled overfeeding studies provide strong evidence against that claim, since people gain very different amounts of weight when overfed the same amount, and some people even lose weight. At low levels of overfeeding, people at normal weight often don’t gain any weight at all.
Another sub-hypothesis is that gaining weight is easy and losing weight is hard, and that consequently that willpower is the main driver of differences in people’s weight. Again, the overfeeding studies seem to contradict this. These people find gaining weight hard and losing weight easy. Notably, they go back to almost exactly their original weight when the study is over. Depending what you mean by CICO, this seems like evidence against CICO (calorie intake ends up being irrelevant in the long term) and evidence in favor of the lipostat perspective (the body will do whatever it needs to bring body weight back to the intended target). But this may not be what most people mean by CICO.
Another sub-hypothesis is something just like, calories are causally involved in weight change. We think this one is true, but just because calories are causally involved doesn’t mean they’re the “first cause”, the cause we should be looking at. Imagine there were an evil dictator that went around force-feeding people. These people would gain weight (per the overfeeding studies) and in some sense the calories would cause the weight gain. But for any reasonable person, the insane dictator is the cause, and the calories are just the mediator. We know people do eat a bit more today than in the 1970s. So the question is something like, in this case, what is the insane dictator? When we say “not CICO” part of what we mean is “not willpower”. But as you can see, this can be a little hard to disentangle! Hope this sheds some light on it, happy to discuss more.
LikeLike
My naive understanding was always “Fat mass uses x calories/kg/day and fat-free mass uses y calories/kg. Your weight is the stable equilibrium between this basic energy use and your food intake.”
Now that I’m looking it up, I see that there’s probably a big constant in energy expenditure. https://en.wikipedia.org/wiki/Basal_metabolic_rate . So I guess I would expect x% more calories to translate to 2x% or an even larger multiple of weight gain. The fact that it translates to 0.5x% is pretty surprising.
The sub-hypotheses of CICO that I endorse are
1) Calories are reasonably substitutable between foods. You might “absorb” x calories from 100 calories of cake and 2x calories from 100 calories of beef but not like 10x.
2) An individual’s stable weight (and hence weight gain) are monotone functions of caloric intake, holding exercise constant. If you keep increasing or decreasing caloric intake you can make yourself gain or lose weight.
LikeLike
Can you explain “not willpower” a little bit more?
LikeLike
I’m still mystified by your position here . 400 extra calories a day is 40 pounds a year assuming you absorb all of the calories, we don’t absorb all of the calories so it only translates to 5 pounds more a year. There are some metabolic factors so in the short term your weight will rebound down or up if you over or under eat. It’s crazy that consuming enough energy to store 40 pounds of fat a year to you is “not too many extra calories”
LikeLike
>The only weakness in the theory is that it’s not clear what could cause the lipostat to be set to the wrong point.
processed fats
LikeLike
I am currently reading ‘Why We Sleep’ and it seems very relevant. Healthy amounts of sleep regulate hunger and satiation, and lack of sleep interferes with both, and a lot of other health parameters as well. May be obesity epidemic is tightly linked with sleep deprivation epidemic?
LikeLike
Possibly — we don’t know much about sleep but you may be interested in Alexey Guzey’s review of that book, which concludes that Why We Sleep is “Riddled with Scientific and Factual Errors”. Judge for yourself: https://guzey.com/books/why-we-sleep/
We do suspect there are interesting relationships between hunger and sleep (and other drives) but that’s an idea for another post.
LikeLike
Thank you for the link. I had no idea this book has so many serious problems!
LikeLike
You’re welcome!
LikeLike
It’s a bit amusing that you are citing Guzley as a model of seriousness; here is a quote from the very page you linked to:
—————————
However, let me make an analogy: when people don’t restrict their food-eating, many of them start eating more than they need and become obese, meaning that simply allowing ourselves to get as much food as we want, likely isn’t the healthiest choice.
—————————
🙂
LikeLike
Haha we noticed that one too! Hopefully we will convince Guzey otherwise. 😉
LikeLike
I have heard that African American women suffer from higher obesity rates. Could obesity be related to the price of food and the lack of availability of high quality food to poor households? After all people eat what they buy and they buy what they can afford and is available close by. Maybe proximity to certain stores is a predictor for obesity.
LikeLike
Have somebody checked a correlation between breast feeding vs. infant formula in early infancy and hungry feelings in adulthood (or weight as a proxy of that)?
It’s just an random idea, but it seems to me that the timeline of increasing obesity and increasing of use of infant formula could be correlated.
LikeLike
Hm, that’s a very interesting idea. It doesn’t seem like the obesity epidemic is entirely developmental but there does seem to be a developmental element, so that could be part of it! We’ll look into it. 🙂
LikeLiked by 1 person
slimemoldtimemold’s posts are getting a lot of attention here (though, sadly, most of the comments are not especially insightful): https://www.metafilter.com/192025/A-riddle-sauted-in-a-mystery-deglazed-with-an-enigma
LikeLike
Incidentally I am bingeing (pun intended) on “low carb down under” talks on YouTube. One speaker was explaining his own hypothesis of how increase in vegetable oils high in poly unsaturaed fats like canola oil, soy oil (he especially mentioned linoleic acid) correlates to increase in obesity. He was even showing the carb vs obesity graph (similar to what you showed) and then overlaying PUFA usage vs.. Obesity graphs to drive his message home. Basically he is saying, saturated fats (and some unsaturated fats like Olive oil to some extend) triggers a mechanism in the cell membrane causing increased insulin resistance of that single cell which after some time that particular cell becomes highly insulin resistant and can’t accept anymore nutrients. In contrast PUFAs don’t trigger this mechanism (details escape me, but it’s about proton pump mechanism on the cell membrane) and no insulin resistance is triggered. This causes the fat cell to grow much bigger. At some points it starts “ejecting” lipids to outside of the cell to avoid bursting and that’s why we see lots of lipids in intra-celluar space and veins in obese people. Those lipids summon macrophages and causes eventually chronic inflamation.
So you are saying something sets the thermostat too high. He says, something (PUFA) interferes with the temperature sensor itself and the cells “think” it’s still too cold and doesn’t stop nutrient intake. Maybe both play a role. You set the thermostat to 72 but you still feel cold but in reality your feeling of coldness is broken. So you begin to crank up the set point slowly (more insulin), which just increases your problems.
I’ve found this hypothesis particularly interesting. What’s your thoughts on that?
P.S. Well, I just searched the youtube to find that talk, but couldn’t. I need to begin taking notes of interesting talks.
LikeLiked by 1 person
+1 to looking into PUFAs. You may be thinking of the talks by Dr. Chris Knobbe: https://www.youtube.com/watch?v=pHnPinYI2Yc and https://www.youtube.com/watch?v=7kGnfXXIKZM (I posted these links in a reply to a comment on Part 1 as well)
LikeLike
Has anybody experimented with the effects of different CO2 concentrations on the lipostat set point?
LikeLike
Hi.
Thank you so much for writing this. I basically just had all my beliefs(which I thought were at least somewhat founded in science) thrown out the window, for the most part. It’s great!
I always figured CICO was the obvious “winner” simply due to, well, common sense, or maybe the laws of physics. Fat gained = Energy eaten – energy spent, more or less. Of course, I figured the real truth must be a lot more complicated(macros and their proportions must play some role). But I did think that CICO was basically what it was all about.
Do you think that food additives such as preservatives could be a part of this? It seems there is a noticeable upwards shift around 1976-1980 in obesity and even a slight upwards trend prior to that. I have no idea when we really started using additives heavily, but even if it weren’t exactly additives, it wouldn’t surprise me if the root cause lay with some kind of “engineering” or processing we are doing to our food in modern times which we didn’t do before. Advancement in food science and technology could then explain the trend, as well as the upticks, if we started doing something drastically different in those periods.
LikeLike
One thing that I’m still confused by: In this post, you knock down just about every hypothesized diet-based explanation, and then conclude that we should look somewhere other than our diet. But in the previous post, you said that rats are observed to get much fatter on “palatable human food” than on other forms of high-fat diet. That seems like pretty strong evidence that it’s something in the food.
Any explanation that says “it’s not our diet, it’s [the environment, the microbiome, whatever]” has to explain why the human diet seems to be so effective at causing obesity in animals – even animals in a lab environment where the diet ought to be the only variable affecting them.
LikeLike
This is a great question! It may be something in the food that is not “diet”, that is not a nutritional feature of the food. Stay tuned and see if the next installments satisfy you on this point.
LikeLike
Pesticides? That would be the only thing missing ingredient from previous/historic populations you mention, as well as a chemical factor in our food.
LikeLike
Is there any reliable geographic data showing where obesity started to rise in the ’76-’80 time frame?
I found myself thinking of a paragraph I read in a Kevin Drum article a while ago, discussing how the pattern of the spread of a phenomenon can suggest where to look for its cause:
“Experts often suggest that crime resembles an epidemic. But what kind? Karl Smith, a professor of public economics and government at the University of North Carolina-Chapel Hill, has a good rule of thumb for categorizing epidemics: If it spreads along lines of communication, he says, the cause is information. Think Bieber Fever. If it travels along major transportation routes, the cause is microbial. Think influenza. If it spreads out like a fan, the cause is an insect. Think malaria. But if it’s everywhere, all at once—as both the rise of crime in the ’60s and ’70s and the fall of crime in the ’90s seemed to be—the cause is a molecule.”
https://www.motherjones.com/environment/2016/02/lead-exposure-gasoline-crime-increase-children-health/
LikeLike
Is there any reliable geographic data on how obesity spread since ’76-’80?
As I was reading, I was thinking of this paragraph from a Kevin Drum piece I read a while ago, talking about how the pattern of spread can give you insight into origins:
“Experts often suggest that crime resembles an epidemic. But what kind? Karl Smith, a professor of public economics and government at the University of North Carolina-Chapel Hill, has a good rule of thumb for categorizing epidemics: If it spreads along lines of communication, he says, the cause is information. Think Bieber Fever. If it travels along major transportation routes, the cause is microbial. Think influenza. If it spreads out like a fan, the cause is an insect. Think malaria. But if it’s everywhere, all at once—as both the rise of crime in the ’60s and ’70s and the fall of crime in the ’90s seemed to be—the cause is a molecule.”
https://www.motherjones.com/environment/2016/02/lead-exposure-gasoline-crime-increase-children-health/
(apologies of this double posted, had to dust off my wordpress profile…)
LikeLike
Hmmm that’s a good question! We can’t find much good state- our county-level data, but Our World in Data has pretty good country-level data going back to 1975: https://ourworldindata.org/obesity
That might be too high-level to detect the spread patterns you’re describing, though… county-level data might be necessary. If anyone has that data, let us know!
LikeLike
“Contrary to stereotypes, more than 50% of Americans meet the HHS guidelines for aerobic exercise. ”
This requires a citation. The HHS itself reports:
“Although the latest information shows some improvements in physical activity levels among American adults, only 26 percent of men, 19 percent of women, and 20 percent of adolescents report suffcient activity to meet the relevant aerobic and muscle-strengthening guidelines”
Click to access Physical_Activity_Guidelines_2nd_edition.pdf
LikeLike
Does obesity correlate to the use of plastics? Especially plastics that come in contact with food or whose volatiles somehow find their way into people’s metabolism?
One fundamental difference between a lifestyle in a modern society and that of a hunter gatherer is the stuff and chemicals that surround people in places with high obesity rates. Stuff that comes into close contact with them. Additives in plastics come into mind. But even consumer products constantly leak volatile organic compounds. Their number in each household has increased, so has the variety of chemicals used in the manufacturing of them and so has indoor ventilation decreased at the same time due to higher insulation and air tightness of modern houses to combat CO2 emissions.
Studies suggest that highly processed food play a major factor in developing diabetes and obesity, yet all the mentioned studies don’t seem to point at the food itself as the culprit. Maybe if it’s not the content then it’s the containers these foods are sold in? Meals that you prepare yourself from raw ingedrients don’t tend be wrapped in as nearly as much plastic as things like ready meals.
So how much did cooking habits change since the 1970s and does it correlate with the obesity rate? What about snacking at places like Subway, people tend to eat at those places more, don’t they? But how do they store their ingredients compared to a diner in the 50-70s?
LikeLiked by 1 person
Hello! I’d like to start off by thanking you a lot for this! My mother and I are currently trying to lose fat and keep it off. I m about five six and a half and somewhere between 130-140 lbs. Since I’m south Asian its a harder effort for me to lose belly fat….
Your pair of articles resonates very strongly with me because I’ve noticed absurdly this. Sometimes when I over eat I just dump it out the next day with not too much weight gain…..
I recently did a six day water fast which seems to have dropped the set point somewhat though I’m not absolutely sure
In any case could it be the same thing in implicated in the drop in testosterone and sperm levels? Namely microplastics? Going to buy a lifestraw filter today just in case that’s the real cause….can’t take any chances.
Its very worrisome but as someone whose paid attention to these debates a lot I have to say you really smashed my assumptions to pieces. I recently jumped from keto to Cico after reading herman pontzer discuss how hadza burn the calories we do but now I’m just not sure.
Anyways I hope you do narrow in on a solution and just from personal experience it does seem to me my body at least has a set point at whatever weight although that set point itself seems to change for reasons unclear so far
LikeLike
We’re so glad you found it meaningful! Like you say, the conversation around weight can be kind of absurd. The bottom line is that it’s very hard to have control over your weight!
Part III should be up soon, so you can take a look at our proposed explanation and see what you think! We’re not sure that a filter will help but it probably won’t hurt.
LikeLike
I can sense where this is going…but I’ll bite my tongue.
LikeLike
First off, thank you very much for the fascinating series—I’m looking forward to the next post!
I want to push back a little on the controlled overfeeding section, which seems to underpin your CICO criticism. I am confused because there is a large natural experiment that has been running for decades which directly contradicts this: the weightlifting/bodybuilding subculture. In this population, people eat carefully tracked caloric surpluses to gain weight (typically 250-500 calories), followed by controlled deficits to cut weight. And this works extremely well, independent of any up or down-regulation of TDEE.
So this statement: “A person at a healthy weight has to eat huge amounts of calories to gain even a couple pounds” doesn’t ring true to me at all. Most people can predictably manipulate their weight up or down by eating a modest caloric surplus/deficit; so-called ‘hardgainers’ who struggle to gain weight invariably turn out to not be consistently eating at a surplus, or failing to track their calories with enough accuracy.
The second statement: “After the overfeeding stops, people go right back to the weight they were before the experiment” I absolutely buy (and have experienced myself), for all the reasons you mention to do with setpoints and homeostasis.
The crucial difference is that out in the real world, the overfeeding never stops. You mention that a 456 increase in daily calorie intake is “quite small”, but I don’t understand your thinking here. That’s enormous! In the lifting community, that would be considered an aggressive-ish bulk, leading to something like a 0.5% increase in bodyweight every week. Unless it’s accompanied by an enormous increase in TDEE, it would easily explain the trend and then some. And if you did it over a period of years (the overfeeding studies are pretty short) it doesn’t seem at all surprising that your setpoint would shift higher.
Perhaps there are confounding factors to do with body composition (a 50/50 split of fat and lean mass gained is typical for lifters, which is probably quite different to the overfeeding studies). But I can’t help but feel like you’re being a little quick to dismiss boring old CICO here.
The other red flag is the stuff around George Bray and some of the prisoners eating 10,000 calories a day. Without having looked at the research, this makes me immediately skeptical of any other claims being made.
A 5000 calorie bulk is challenging for the average person, even using ‘dirty’ strategies. If you go out and try to eat 10,000 calories in one day, and you are not a 200kg professional strongman, you will discover that is damn near physically impossible to do so, let alone repeat the feat daily over a course of weeks or months. These kind of claims are almost certainly hyperbole or measurement error—for example, Ian Thorpe’s legendary 12,000 calorie intake was a total myth, but it endures long after his repeated disavowals.
Obesity crisis is prob not monocausal but I’m not ready to throw out the simplest underlying explanation. Aware I am probably missing something, would love to hear your further thoughts and thanks again for the great deep dive.
LikeLike
First off, thank you very much for the fascinating series—I’m looking forward to the next post!
I want to push back a little on the controlled overfeeding section, which seems to underpin your CICO criticism. I am confused because there is a large natural experiment that has been running for decades which directly contradicts this: the weightlifting/bodybuilding subculture. In this population, people eat carefully tracked caloric surpluses to gain weight (typically 250-500 calories), followed by controlled deficits to cut weight. And this works extremely well, independent of any up or down-regulation of TDEE.
So this statement: “A person at a healthy weight has to eat huge amounts of calories to gain even a couple pounds” doesn’t ring true to me at all. Most people can predictably manipulate their weight up or down by eating a modest caloric surplus/deficit; so-called ‘hardgainers’ who struggle to gain weight invariably turn out to not be consistently eating at a surplus, or failing to track their calories with enough accuracy.
The second statement: “After the overfeeding stops, people go right back to the weight they were before the experiment” I absolutely buy (and have experienced myself), for all the reasons you mention to do with setpoints and homeostasis.
The crucial difference is that out in the real world, the overfeeding never stops. You mention that a 456 increase in daily calorie intake is “quite small”, but I don’t understand your thinking here. That’s enormous! In the lifting community, that would be considered an aggressive-ish bulk, leading to something like a 0.5% increase in bodyweight every week. Unless it’s accompanied by an enormous increase in TDEE, it would easily explain the trend and then some. And if you did it over a period of years (the overfeeding studies are pretty short) it doesn’t seem at all surprising that your setpoint would shift higher.
Perhaps there are confounding factors to do with body composition (a 50/50 split of fat and lean mass gained is typical for lifters, which is probably quite different to the overfeeding studies). But I can’t help but feel like you’re being a little quick to dismiss boring old CICO here.
The other red flag is the stuff around George Bray and some of the prisoners eating 10,000 calories a day. Without having looked at the research, this makes me immediately skeptical of any other claims being made.
A 5000 calorie bulk is challenging for the average person, even using ‘dirty’ strategies. If you go out and try to eat 10,000 calories in one day, and you are not a 200kg professional strongman, you will discover that is damn near physically impossible to do so, let alone repeat the feat daily over a course of weeks or months. These kind of claims are almost certainly hyperbole or measurement error—for example, Ian Thorpe’s legendary 12,000 calorie intake was a total myth, but it endures long after his repeated disavowals.
Obesity crisis is prob not monocausal but I’m not ready to throw out the simplest underlying explanation. Aware I’m probably missing something, would love to hear your further thoughts and thanks again for the great deep dive.
LikeLike
First off, thank you very much for the fascinating series—I’m looking forward to the next post!
I want to push back a little on the controlled overfeeding section, which seems to underpin your CICO criticism. I am confused because there is a large natural experiment that has been running for decades which directly contradicts this: the weightlifting/bodybuilding subculture. In this population, people eat carefully tracked caloric surpluses to gain weight (typically 250-500 calories), followed by controlled deficits to cut weight. And this works very well indeed, independent of any up or down-regulation of TDEE.
So this statement: “A person at a healthy weight has to eat huge amounts of calories to gain even a couple pounds” doesn’t ring true to me at all. Most people can predictably manipulate their weight up or down by eating a modest caloric surplus/deficit; even the ‘hardgainers’ who struggle to gain weight invariably turn out to not be consistently eating at a surplus, or failing to track their calories with enough accuracy.
The second statement: “After the overfeeding stops, people go right back to the weight they were before the experiment” I absolutely buy (and have experienced myself), for all the reasons you mention to do with setpoints and homeostasis.
The crucial difference is that out in the real world, the overfeeding never stops. You mention that a 456 increase in daily calorie intake is “quite small”, but I don’t understand your thinking here. That’s enormous! In the lifting community, that would be considered an aggressive-ish bulk, leading to something like a 0.5% increase in bodyweight every week. Unless it’s accompanied by an enormous increase in TDEE, it would easily explain the trend and then some. And if you did it over a period of years (the overfeeding studies are pretty short) it doesn’t seem at all surprising that your setpoint would shift higher.
Perhaps there are confounding factors to do with body composition (a 50/50 split of fat and lean mass gained is typical for lifters, which is probably quite different to the overfeeding studies). But I can’t help but feel like you’re being a little quick to dismiss boring old CICO here.
The other red flag is the part about George Bray and some of the prisoners eating 10,000 calories a day. Without having looked at the research, this makes me skeptical of any other claims they’re making.
A 5000 calorie bulk is challenging for the average person, even using ‘dirty’ strategies. If you go out and try to eat 10,000 calories in one day, and you are not a 200kg professional strongman, you will discover that is damn near physically impossible to do so, let alone repeat the feat daily over a course of weeks or months. These kind of claims are almost certainly hyperbole or measurement error—for example, Ian Thorpe’s legendary 12,000 calorie intake was a total myth, but it endures long after his repeated disavowals.
Obesity crisis is prob not monocausal but I’m not ready to throw out the simplest underlying explanation. Aware I’m probably missing something, would love to hear your further thoughts and thanks again for the great deep dive!
LikeLike
This is a set of really sophisticated questions, thank you for bringing these up!
Part of the problem is that CICO means different things to different people, and covers a number of loosely related hypotheses. We found it hard to disentangle these when writing the post but feedback like yours is proving helpful.
One way to interpret CICO (or one sub-hypothesis) is that it claims there is a strictly LINEAR relationship between calories eaten/burned and weight change. This is specified if we take “weight gain = calories in – calories out” literally. This is clearly false. The overfeeding studies provide extremely strong evidence against this version of CICO, since people gain very different amounts when overfed, the difference appears mostly genetic, and some people actually lose weight when overfed by small amounts. Many people still believe something like “for every extra 3500 calories you eat you always gain one pound”, but all available evidence comes down very strongly against that.
Another interpretation of CICO (though less explicitly spelled out) is that weight gain is easy and weight loss is hard for everyone. This interpretation says something like, everyone would be 300lbs if they didn’t use their willpower to eat healthy foods rather than cake, you have to control yourself. From this perspective, people who are obese lack willpower and people who are thin/fit are virtuous resisters of temptation. The overfeeding studies also provide strong evidence against this, since they find that it is hard for most people to gain weight and easy for them to go back exactly to where they were at before the overfeeding. We think this leaves “willpower” explanations dead in the water. Also we eat all the cake and ice cream (etc.) we want and neither of us are obese.
Another interpretation is something like, calories matter for weight gain. We are not trying to argue against this at all! If you eat 400kcal/day, you will lose weight. If you eat 10,000 kcal/day, you will gain weight. But the amount of calories you eat matters much less than most people think, and there isn’t a strong linear relationship between calories consumed and weight gain.
We think a 456 increase in daily calorie intake is small compared to what we see in controlled overfeeding studies (also FWIW it was smaller than we expected), but you may be right, the long-term effects could be large. Two points about this, however. There’s some evidence that back around 1900 people ate this much or more daily, without much more exercise, and they weren’t obese (take this one with a grain of salt since we don’t have great calorie data from back then). Second, even if the increase is meaningful and driving the obesity epidemic, we have to ask, why are people eating more now than they used to? We think “CICO” implies “willpower” to most people, and as we said, we don’t think that explanation holds water.
We also suspect that weight gain and loss may work differently in bodybuilding because that involves weight change driven by increases in muscle mass, not fat mass. We’re perfectly willing to believe that people can gain and lose muscle mass (and associated fat mass?) in a reliable way based in part on caloric consumption, but that’s also not the focus of the piece. Cutting fat gained when increasing muscle mass might also be relatively easy because that’s more fat than you “naturally” had before the gains. Changing fat mass alone seems pretty hard. So we might qualify that as, “A person at a healthy weight has to eat huge amounts of calories to gain even a couple pounds *of fat*”
Hopefully this clarifies, let us know what you think!
LikeLike
Thanks a lot for the thorough response, this helps a lot to pin down where we might actually disagree. We’re definitely on the same page re: the correct interpretation of CICO: number of calories entering mouth ≠ net energy entering the system because of variance in digestion, changes in TDEE, etc. The body is not a bomb calorimeter.
Hard agree on the willpower argument too. All the evidence I’ve seen is that losing weight and *keeping it off long term* is vanishingly rare, and involves a grinding Sisyphean battle against one’s own metabolism and endocrine system. If shaming/social stigma/’don’t be lazy’ actually worked, we would be seeing very different results.
Which leaves us with the increase in daily calorie intake. I’m not going to dismiss the 1900 data as unreliable without knowing the methodology, but my prior is that basically all reported calorie intake is suspect unless collected under extremely careful conditions (self-reporting in particular is infamously inaccurate). I don’t know what methodology the Pew or other studies used either, so I guess it could skew in either direction.
If it turns out that the Pew data is more or less correct, my guess is that is sufficient to explain the epidemic on a strict CICO level. But as you point out, that doesn’t answer the question of what is actually __causing__ the increase in calorie intake!
A thought I had while reading through your article, and thinking back to Guyenet’s book: I wonder if there’s any way to measure an increase in the variety of food sources? As in, it’s not just that food became cheaper, tastier, and more readily available, but that there’s also a much broader range to choose from at any given moment? Kind of like the Coolidge effect but for food.
Like I said before I doubt it’s monocausal, so I’m looking forward to reading the next installation.
LikeLike
> We also suspect that weight gain and loss may work differently in bodybuilding because that involves weight change driven by increases in muscle mass, not fat mass.
This is wrong. After the first, say, 12 months of consistent lifting with adequate protein, gaining more muscle becomes notoriously slow (certainly far less than 1 pound per month), and anyone who’s gotten to the point of being a *professional* bodybuilder is very close to their “genetic ceiling” of how much muscle they can put on their frame. At that point, changes in bodyweight are almost entirely fat, with muscle gains and losses being hard to distinguish from rounding error in comparison.
LikeLike
My understanding is that, when a person loses weight, the total number of fat cells does not change by much, could it be that overeating as a kid makes it really difficult to lose weight as the body has no mechanism of fat cell elimination? (or a really slow mechanism/a mechamism that would only come into play long after people simply stop dieting, making their emptied fat cells fill back up) would sorta work with the thermostat theory, at least on the side of weight loss being difficult, explain why it looks genetic even though genes haven’t changed, but not explain why for example the people of japan become fat when they move to the US, which is super weird because earlier you said people simply go back to their original weights.
LikeLike
> Pew says calorie intake in the US increased from 2,025 calories per day in 1970 to about 2,481 calories per day in 2010. The USDA Economic Research Service estimates that calorie intake in the US increased from 2,016 calories per day in 1970 to about 2,390 calories per day in 2014. Neither of these are jaw-dropping increases.
These are absolutely jaw-dropping increases, it’s 20% of calories! If anything, it’s surprising people aren’t getting more obese.
I’m holding calories-in calories-out to be mostly true. I ran the experience on myself, tracking calories in via MyFitnessPal and calories out via Fitbit, and then making a weight loss prediction. The model turned out to be surprisingly accurate (I wouldn’t expect it to be so accurate with everyone). At the very least this strongly reinforced my confidence in the model.
Lipostat is a neat explanation of why people revert after a diet. We know all diets work, but out of the diet, people tend to revert. I don’t think it’s even that diets are too hard to maintain, it’s the small subtle nudges that end up adding up. A chocolate bar here and a small bag of chips there add up very very quickly – even though it doesn’t feel like splurging. Only constant vigilance (not sacrifice) saves you if you’re prone to diet reversal.
I think the missing explanation might be palatability and ease of access. These days, it’s easy to get a snack anytime anywhere, and they taste damn good. They’re also varied. Sure, honey is sweet, but if you get 60% of your calories from honey, you’re much less prone to think “hhm, I sure could use a honey snack”. And even less if you actually have to collect the honey, or if the reserves are limited.
Small psychological tricks like keep your snacks in hard to reach place, or getting rid of them entirely work well, for that reason. Another strategy is to limit variety in the diet.
LikeLike
This is a very interesting analysis, and thanks very much for the detail. One thing did stick out:
‘The USDA Economic Research Service estimates that calorie intake in the US increased from 2,016 calories per day in 1970 to about 2,390 calories per day in 2014. Neither of these are jaw-dropping increases.’
As a couple of other commenters have mentioned, that is a huge increase. In fact, it is certainly large enough to explain all the changes in obesity rate, and without other factors would cause a much WORSE obesity problem than we currently have.
An excess of 374 calories per day is around 135 Mcal per year (taking 1cal=4.2kJ). If we assume that people in 1970 and 2014 have identical total energy expenditure, individuals in 1970 maintained a steady weight, and that this excess energy is stored efficiently as fat, then that corresponds to a weight gain of more than 9 kg (20lb) per year.
Even a one-off weight gain of 9kg for a male individual of average height and BMI 23 (175cm, 70kg) would put them in the overweight category (BMI 26) and doing it three times in the obese category. If this individual gained 20 pounds a year for 45 years, they would be pushing 1000 pounds. And, under the assumptions above, this would be the AVERAGE weight gain for an American individual over their life.
Needless to say, the average American is not gaining 9kg (20lb) per year!
All of the compensatory mechanisms you mention are very valid and interesting – but it feels like, rather than debunking theories of why people are obese, they are all strongly contributing to reasons why people aren’t much MORE obese than they actually are.
In other words, the question isn’t ‘why are we fat, despite not eating much more?’ but ‘given how much more we eat, why aren’t we all human beach-balls?’
LikeLiked by 1 person
While the The Bland Food Cookbook, the premise of more rewarding foods throwing the “lipostat” out of whack seems absurd when one considers French cuisine and their historical body composition/health. At the very least it isn’t a question of taste!
LikeLike
While the The Bland Food Cookbook is an April Fools joke, the premise of more rewarding foods throwing the “lipostat” out of whack seems absurd when one considers French cuisine and their historical body composition/health. At the very least it isn’t a question of taste!
LikeLike
Yeah, good point!
LikeLike
Not necessarily, if it is the combination of food companies’ perfecting the ability to trigger reward via taste and the quick digestion from heavily processed foods. The theory is based on the amount of reward and in the time difference between the detection of taste and the detection of glucose. In most cases (like french cuisine) the difference in set point may be minimal, but in the unnaturally extreme cases of junk food and fast food the set point may increase dramatically. And if I recall correctly, the one consistent finding in obesity research is that junk food and fast food increase weight gain.
LikeLike
I suggest the “bland food” theory receive a bit more examination. Nothing in the article gives evidence that the lack of association with rewarding taste doesn’t affect weight gain. The theory is that the stronger the association (meaning the co-incidence of strong rewarding taste with calorie detection) with rewarding taste, the more the body thinks we are in a time of harvest and should load up on calories. More quickly digested glucose increases the association because the time of taste and time of glucose detection is shorter. So more heavily processed foods with stronger, more rewarding taste (ie., junk food, fast food) increase the set point the most. And studiees do show that junk food and fast food are related to obesity, correct? Also, I believe a small number of studies show that ingesting tasteless calories taken at least an hour before and after eating anything with taste decreases the set point, even though calorie intake went up. Might look into that.
LikeLike
I’m reading the late Seth Roberts’ book “The Shangri-La Diet” now. The foundation is the lipostat idea — he theorizes that the body has a set point that the body “wants” to be. He thought the set point is pushed up when our calories become associated with lots of flavor, and can be pushed down when our calories become associated with less flavor. So if I eat 1000 calories a day of Twix bars, I’ll become much hungrier than my twin who eats 1000 calories a day of vegetables and baked chicken.
The reason I thought to post this is that it would help explain the altitude phenomenon. If altitude reduces flavor, and a quick Google search makes that seem possible, then this theory would predict that people in low altitudes would end up with higher set points than people in high altitudes.
It still doesn’t offer an explanation for the spike in obesity starting in 1980.
Thank you for all your work on this!
LikeLike
[…] but this is not because the diets stop working, but because the people stop following the diets.In part ii of the series, the author calls into question the calories in vs calories out […]
LikeLike
I tend to agree with @Benjamin Kadish
“It’s true that people eat more calories today than they did in the 1960s and 70s, but the difference is quite small. Sources have a surprisingly hard time agreeing on just how much more we eat than our grandparents did, but all of them agree that it’s not much. Pew says calorie intake in the US increased from 2,025 calories per day in 1970 to about 2,481 calories per day in 2010. The USDA Economic Research Service estimates that calorie intake in the US increased from 2,016 calories per day in 1970 to about 2,390 calories per day in 2014. Neither of these are jaw-dropping increases.”
Surely that extra ~400 calories – if not used – could cause someone to gradually gain weight over time until they were obese?
They would not become obese overnight but the sustained calorie surplus over months/years would cause them to slowly gain weight until they were obese?
And maintaining that calorie surplus would cause them to remain obese?
And, as an obese body requires more calories, the body produces urges to eat even more calories – leading to a vicious cycle of increased calories and weight?
LikeLike
Haven’t read your entire series of articles yet, but you may want to further explore the connection between appetite and altitude before you make too many assumptions about it in your obesity theories. Altitude affects appetite in that it reduces one’s ability to smell and taste. People and animals at higher altitude desire to eat less overall.
Airline food has been long known to suffer from this issue.
LikeLike
I’m a practicing Bariatric Surgeon. A patient of mine recommended ACH to me. I love it. Well done.
One thing, the gastric bypass is far too elegant to be compared to property damage. 😉
LikeLike
Thank you! 😀
You’re right, surgically Roux-en-Y is a work of art
LikeLike
You briefly mention smoking rates and all of the examples you offer indicate higher rates of smoking accompanying lower BMI. Then you dismiss this as a possible explanation based on rates of hypertension. This seems to be a non sequitur.
LikeLike