
The potato diet is a diet where you get most or even all of your calories from potatoes. Surprisingly, this is easy for many people to stick to, and participants who stayed on the diet for a full 28 days lost an average of 10.6 lbs, despite the fact that nearly all of them took multiple cheat days. This seems like a pretty strong weight loss effect, but the question remains: why does it work?
Potatoes are special for many many reasons, but by far the most obvious thing that makes them special is that they’re really high in potassium. If potassium is the reason the potato diet makes people lose weight, then there’s a good chance that taking potassium directly would also make people lose weight. Someone should really do a study. Who, us? Ok, fine.
Tl;dr, we’re looking for people to volunteer to supplement small doses of potassium chloride (KCl) for at least four weeks, and to share their data so we can do an analysis. You can sign up below.
Potassium
Potassium (K) is a slivery-white alkali metal, and element number 19 on the periodic table. In its pure form, it is highly explosive on contact with water. But most of the time, we encounter potassium in forms where it is much more stable.
In these non-explosive forms, potassium is an essential mineral for human life. Because it plays many important roles in your biology, you have to consume a small amount of potassium every day to remain healthy.

Megadoses
There are a couple reasons to suspect that potassium might be the active ingredient driving the weight loss we see on the potato diet. The first is that the potato diet provides stunningly high doses of potassium, amounts that most people would never otherwise consume.
For a long time, the recommended daily value for adults (technically, the “Adequate Intake”) was 4,700 mg of potassium per day. But most people don’t get anywhere near this amount.
In every CDC NHANES dataset from 1999 to 2018, median potassium intake hovers around 2,400 mg/day, and mean intake around 2,600 mg/day. In this report from 2004, the National Academy of Medicine found that “most American women … consume no more than half of the recommended amount of potassium, and men’s intake is only moderately higher.” Per this paper, only 0.3% of American women were getting the recommended amount. Similarly low levels of intake are also observed in Europe, Mexico, China, etc.
But in 2019, the National Academies of Sciences, Engineering, and Medicine changed the recommended / adequate intake to 2,600 mg/day for women and 3,400 mg/day for men. They say that the change is “due, in part, to the expansion of the DRI model in which consideration of chronic disease risk reduction was separate from consideration of adequacy,” but we can’t help but wonder if they changed it because it was embarrassing to have less than 5% of the population getting the recommended amount.
In any case, recommended potassium intake is something like 2,500 to 5,000 mg per day for adults, and many people don’t get enough.
Potatoes are exceptionally high in potassium. A single potato contains somewhere between 600 and 1000 mg of potassium, depending on which source you look at. They are the 6th highest in potassium on this list of high-potassium foods from the NIH, and 9th on this old list from the USDA. If you do the math, this means that someone on the potato diet, eating 2,000 kcal of potatoes a day, gets at least 11,000 mg of potassium per day, more than twice the old recommended intake.
Some people on the potato diet found their appetite decreased so much that they were only eating about 1,000 calories per day — but even then, they would still be getting around 5,500 mg of potassium.
Only 2.8% of Americans in the NHANES data got 5,500 mg per day or more. Only 0.06% were recorded as getting 11,000 mg/day or more. Clearly, the potato diet provides way more potassium than most people would ever get in their day-to-day lives.
Correlational Evidence
One study, published in 2019, looks at the relationship between potassium intake and weight loss. As far as we know, it’s the only study of its kind (if you know of any others, send ‘em our way). In this study, sixty-eight people were enrolled in a “moderate low calorie/high protein Mediterranean diet” for a year. People generally lost weight, and “the strongest correlate of the decline in BMI was the increase in dietary potassium intake.”
In the aggregated publicly-available NHANES data from 1999 to 2018, potassium intake is negatively correlated with BMI (r = -0.055, p < .001) and log BMI (r = -0.051, p < .001). Because of complications around body size (taller people consume more food anyways, and therefore more potassium), we actually think that potassium per calorie, or potassium density, is the more appropriate measure. The relationship here is weaker (r = -0.031 with BMI, r = -0.022 if BMI is log-transformed), but still significant because of the large sample size.
But the really interesting thing is that the relationship gets stronger year-to-year across the span of the NHANES data. Here it is with both BMI and potassium density log-transformed. The relationship holds regardless of transformation, but log-transformation makes for the clearest visualization:
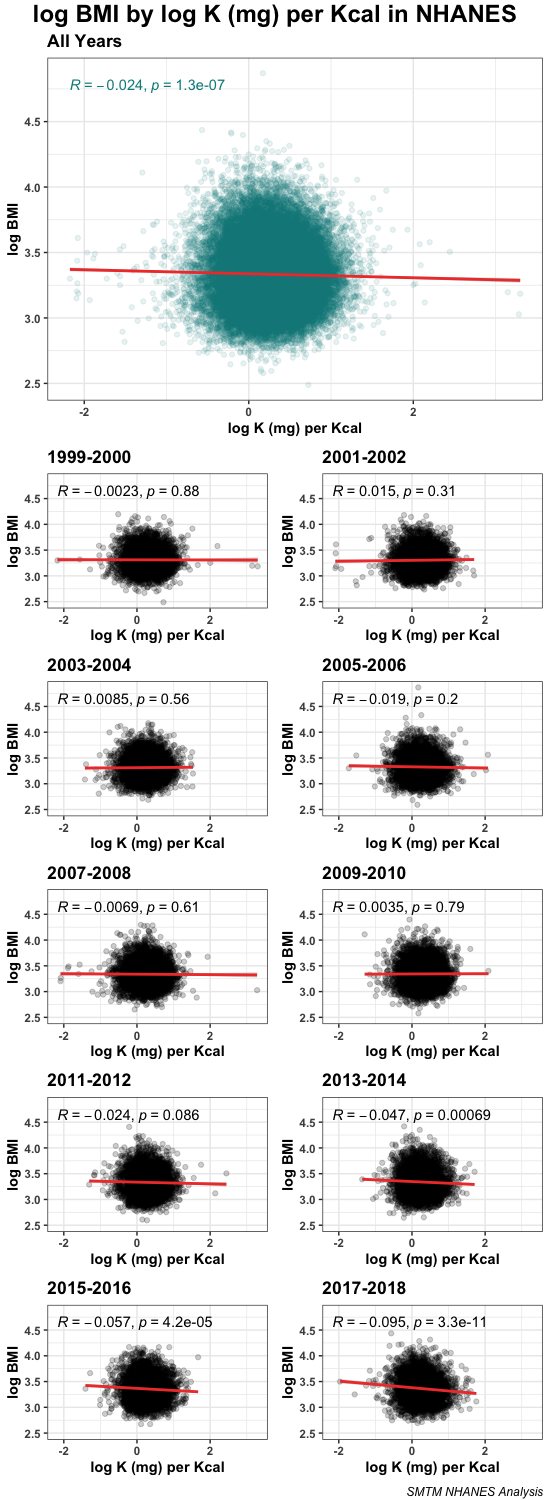
The relationship between potassium density and BMI is not significant in the early years of the NHANES data. From 1999 to 2010, the correlation is always consistent with zero, and p-values are always .20 or greater, even with these very large sample sizes. The sign of the nonsignificant relationship flips back and forth between positive and negative.
But in the 2011-2012 dataset, the relationship is negative, and the p-value drops below 0.10 for the first time. In the 2013-2014 dataset, the relationship is negative and significant (p < .001). In the remaining two datasets, 2015-2016 and 2017-2018, the correlation gets stronger and stronger. By 2017-2018, the correlation is r = -0.095. Aggregated across all years, the relationship is “only” r = -0.024, but that obscures the fact that the correlation has been increasing since around 2011.
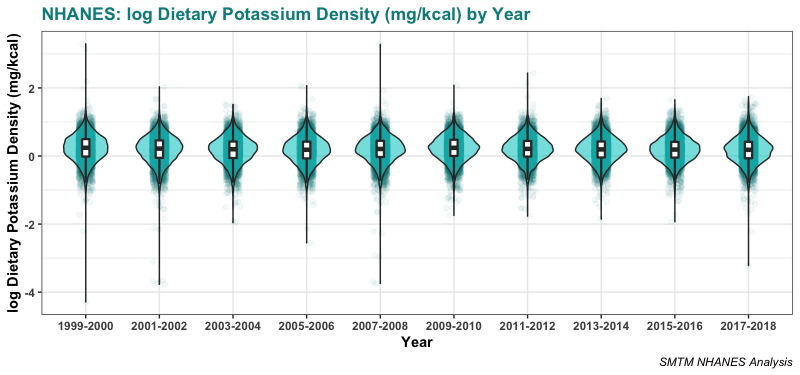
There are certainly alternative explanations for this finding. For example, people who eat a diet that is higher in vegetables might both have lower BMIs and get more potassium on average. But it’s hard to come up with an explanation for why the relationship has been increasing, especially since potassium consumption / dietary potassium density haven’t changed at all over the same timespan:
This analysis doesn’t tell us much by itself. It isn’t strong evidence that potassium can cause weight loss, and doesn’t convince us of anything in particular. But it’s genuinely pretty weird, and since we don’t have much other correlational evidence, we thought it was good to mention.
Self-Experimentation
The final reason to suspect that potassium might cause weight loss is that we tried taking small doses of potassium for a couple of weeks and we lost weight right away.
Two of the SMTM authors did a self-experiment where we took small doses of Nu-Salt and tracked our weight over time. Nu-Salt is just potassium chloride (KCl) in a salt shaker, marketed as a sodium-free alternative to table salt. You can buy Nu-Salt shakers online, at many local grocery stores, or even at Wal-Mart.

We started with two doses of 1/8 teaspoon Nu-Salt (about 330 mg potassium) twice a day and worked up from there. Straight potassium chloride is kind of gross (at least to us, your mileage may vary), so most of the time we mixed the KCl with a drink like Vitamin Water or Gatorade and just chugged it, though occasionally we mixed the potassium into food. Eventually we worked up to doses of 1/2 teaspoon a few (usually 2) times a day.
The first SMTM author to try this lost 5 lbs over the first 10 days, and then hovered around 5 lbs down for the remainder of the four weeks. At the lowest point, they were down 8.4 lbs.
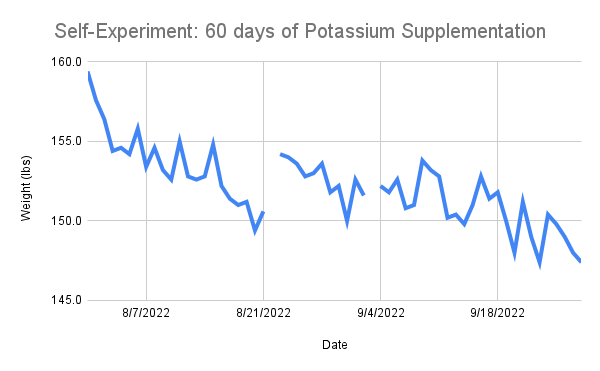
The second author to try potassium supplementation lost 6 lbs over four weeks. They found this so easy that they kept going, and ended up losing a total of 12 lbs over 60 days. Some say they’re still taking potassium to this day (they are).
Here’s the graph for that second author. Note the two gaps when they weren’t able to weigh themselves because they had social commitments — a concert (the first gap) and a fishing tournament (the second gap).
This weight loss is modest, but surprising given that neither of these authors were very heavy to begin with. We also didn’t do anything else to try to lose weight — we weren’t sleeping more or eating better or doing more cardio. All we did was start taking some extra potassium. Honestly we are shocked. This is kind of unbelievable and we need other people to try it because we are so shocked.
Supplementing potassium, even at these low doses, felt a lot like being on the potato diet. From the start, we felt fidgety and sometimes hypomanic.
As on the potato diet, we noticed we needed more salt (i.e. more sodium) and more water, but we didn’t always crave salt or feel thirsty, and we had to consciously eat more sodium and drink more water to avoid feeling bad. A related side-effect is that salty foods like potato chips no longer taste salty — we suspect this is because the body needs so much sodium to balance out the potassium that it has “taken the brakes off” the mechanisms that normally make you stop cramming pickles into your mouth. Even straight table salt didn’t taste overwhelmingly salty.
We eventually figured out that you can put table salt into the same glass of water as potassium salt and drink them at the same time. This helps make sure you’re getting more sodium to balance out the potassium, and it also seems to make the potassium taste less weird.
We mostly did half as much sodium salt as potassium salt, a 1:2 ratio — for example, if we were taking a dose of 1/4 tsp potassium salt in water, we would add 1/8 tsp sodium salt to the same glass. But we’re not sure what the best ratio is, and we notice that some electrolyte powders have much higher ratios. For example, LMNT contains 1000 mg sodium for every 200 mg potassium. This seems like a lot but maybe a 5:1 ratio is better, people seem to like the taste of this stuff.
Like on the potato diet, we found our appetites diminished — what had been regular-sized meals made us feel stuffed like we had just finished Thanksgiving dinner. And just like on the potato diet, what little hunger remained was “weird” and easy to miss.
When we did feel hungry, it didn’t feel like a “problem”, and we sometimes went too long without eating and ended up feeling like crap. Hunger usually manifested as headaches, fatigue, and mood changes, rather than the physical signs we’re used to. Again, this sounds like the potato diet. For reference, this is how some people described the experience of hunger on the potato diet:

(And if it does work like the potato diet, then maybe be on the lookout for other weird side effects, like the intense anxiety reported by a few people.)
All this sounds a lot like the potato diet. But that in itself is kind of mysterious. People on the potato diet were getting about 10,000 mg of potassium a day. In comparison, we never supplemented more than 4,000 mg a day, and started the first day with only 660 mg. So it’s worth musing over why we lost weight on such small small doses.
One possibility is that small amounts of straight potassium salt act as a bolus dose. Potassium in food is essentially a slow-release formulation, but straight KCl in solution might be absorbed much more quickly and directly. This means that relatively small doses of potassium salts may lead to bigger spikes in blood potassium. If potassium causes weight loss by reaching a certain serum level, or by reaching the brain, a bolus may be much more effective than an extended-release formulation, which is what you would get in food.
We were also taking a different form of potassium than is found in food. The potassium compounds found in fruits and vegetables “include potassium phosphate, sulfate, citrate, and others, but not potassium chloride.” Not to mention the fact that we were dissolving the salt into drinks, so really we were getting straight potassium ions, not compounds that needed to be digested.
And in our case, we not only took our KCl in a drink, we tended to chug it all at once. It takes like 5-10 minutes to finish a plate of potatoes; compare that to chugging 330 mg K+ in a Vitamin Water in 10 seconds flat. Even if the potatoes contain more potassium, the pure ions hitting your stomach in such a small window might make a big difference. This might also contribute to a bolus effect.
We also tended to take our first dose early in the day, often before we had eaten our first meal. If potassium suppresses your appetite, you might get more of an effect if you take it before food. If you’re getting your potassium from food, you literally can’t take it before food.
A final explanation is that we were somehow primed for weight loss and weird side-effects from doing potato diet self-experiments. Both authors had been self-experimenting with potato diets before trying potassium supplementation, and it’s possible that after several months of high potato intake, pure potassium has more of an effect. We don’t know enough to say anything with confidence yet. But you know, that’s why we want to do a bigger study.

Theory Viability
An important consideration when thinking about new theories is, if this were true, could we have missed it? For example, we can be pretty confident that cheese doesn’t cure cancer, because if it did, someone probably would have noticed by now (compare XKCD’s The Economic Argument). So in this case we should ask ourselves, if dietary potassium leads to weight loss, could that have really flown under the radar? What are the chances that (almost) everyone would have missed it?
We think it’s possible. The potato diet gives an exceptionally high dose of potassium, much higher than the recommended amount and more than almost anyone is getting in their normal everyday diet. If doses in this range reduce obesity, we probably wouldn’t have noticed because people almost never consume such large amounts on a daily basis.
While there seems to be a relationship with BMI in the normal dietary range, that relationship is hard to detect. The relationship in the NHANES data isn’t even statistically significant until 2013-2014, so people have had less than ten years to notice it. The correlation in the dietary range is also quite small, only about r = 0.05. You need a sample size of 783 observations to have just 80% power to detect a correlation of 0.10, and the correlation between BMI and potassium has never been that high, at least not in the NHANES data. If you want 90% power to detect a correlation of r = 0.05, you need 4,200 observations. So aside from in the NHANES, there haven’t been many chances to notice this either.
Even when people do supplement potassium, they tend to take really tiny amounts. Potassium supplements and multivitamins pretty much always contain 99 mg potassium or less. This appears to be the result of a ruling by the FDA, which says that oral potassium chloride supplements that provide more than 99 mg potassium are unsafe because they have been associated with small-bowel lesions. (This ruling only applies to non-prescription pills; prescription potassium tablets often contain more than 100 mg.)
We can’t quite tell if the FDA has regulated that you can’t put more than 99 mg in a supplement, or if they just require you to add a warning about small-bowel lesions and all the manufacturers have decided not to risk it. The relevant ruling appears to be 21 CFR 201.306, which does not seem to be a regulatory action, but there’s also something in the Federal Register from 1992 (57 FR 18157) which we haven’t been able to find. In any case, this appears to be the origin of the practice.
We are pretty sure that limiting potassium to 99 mg does not make sense and is wrong, for several reasons. First of all, we know that people can handle doses of potassium above 99 mg in some form or another, because people get several thousand mg from their diets every day. And potassium chloride is not the only way to consume potassium. Even if potassium chloride did somehow cause small-bowel lesions, people could take potassium citrate or potassium phosphate instead.
It’s not even clear what the original ruling was based on. This page from the NIH points to this document as a reference for the ruling, but that document just lists “all solid oral dosage form drug products containing potassium chloride that supply 100 milligrams of potassium per dosage unit” under the heading “216.24 Drug products withdrawn or removed from the market for reasons of safety or effectiveness”, and doesn’t give any reason why they were withdrawn.
The original ruling from 1975, 21 CFR 201.306, doesn’t cite any sources, and it is pretty noncommittal about the state of the evidence:
There have been several reports, published and unpublished, concerning nonspecific small-bowel lesions consisting of stenosis, with or without ulceration, associated with the administration of enteric-coated thiazides with potassium salts. These lesions may occur with enteric-coated potassium tablets alone or when they are used with nonenteric-coated thiazides, or certain other oral diuretics. … Based on a large survey of physicians and hospitals, both United States and foreign, the incidence of these lesions is low, and a causal relationship in man has not been definitely established. Available information tends to implicate enteric-coated potassium salts, although lesions of this type also occur spontaneously.
As far as we can tell, this was all prompted by a small number of articles from the 1960s. This article from 1965 reports six cases of “non-specific ulceration of the small intestine presenting as intestinal obstruction, perforation or haemorrhage” in patients taking “Hydrosaluric-K (enteric-coated hydrochlorothiazide with potassium chloride)”.
You’ll notice that both of these sources are saying something much more specific than just “potassium bad”. This article, also from 1965, makes it pretty clear that it thinks that enteric-coated potassium supplements, specifically, are to blame:
In 1957 the first of the group of thiazide diuretics was introduced. Because increased potassium excretion is one of the pharmacological effects of these thiazides, from the beginning of their use the supplementary administration of potassium has been a common procedure for protection against the potentially serious hazard of hypokalemia. In 1959, the first of several combinations of a thiazide diuretic with potassium chloride in a single tablet was introduced; some of these combinations are enteric coated while others are not.
Since 1957 there has been a striking increase in incidence of small-bowel ulcerative lesions. Recognition that these are related to the ingestion of enteric-coated potassium chloride is due primarily to the observations of Lindholmer et al in Sweden and Baker et al in this country.
Enteric coating refers to a polymer barrier applied to a pill or supplement that keeps it from dissolving in the stomach. Pills are coated this way for various reasons, but the end result is that the drug or substance is delivered to the intestines, rather than to the stomach. The second paper here is pretty confident that delivery to the intestine, rather than the potassium salt per se, is the problem. “A new preparation is necessary,” they say, “which will not … release potassium suddenly in the small intestine permitting absorption of a high concentration of the potassium chloride.”
Even with enteric coating, these lesions appear to be pretty rare. In that first set of six case studies, the authors note that, “in view of the widespread use of enteric-coated diuretic and potassium chloride tablets, constricting ulcers of the small intestine must be a very rare complication.” They cite only 53 cases from 1963 to 1965, “in which 48 patients had been taking enteric-coated thiazide and potassium chloride tablets, three patients may have been, and two had not.”
All the original sources seem to make it clear that enteric-coated potassium tablets are the thing to watch out for, not potassium itself. This was preserved in the 1975 ruling (“nonspecific small-bowel lesions … associated with the administration of enteric-coated thiazides with potassium salts”), but somewhere along the way the message was muddled and people got confused, and started thinking any potassium pills were potentially dangerous.
This appears to be a misconception. Though it’s not easy to find in a supplement, people regularly take prescription tablets of more than 100 mg potassium chloride and are just fine. Plain old potassium chloride seems pretty safe, and we can say that with some confidence because it’s something that has been the subject of many studies.
(Sadly none of these studies seem to have tracked body weight.)
In this hypertension study from 1985, participants were given about 2,500 mg potassium a day as “Slow-K (Ciba) eight tablets a day” for a month. They don’t report any negative events.
In this hypertension study from 2005, participants in one arm of the study were given about 3,700 mg potassium a day as “12 Slow-K tablets”. This lasted for a week and as far as we can tell, everyone was ok — they certainly don’t mention any bowel lesions in the paper. [Edit: We missed it the first time around, but this study did track body weight. People in the trial lost an average of 0.1 kg (0.22 lbs) over 7 days on potassium citrate, and an average of 0.3 kg (0.66 lbs) over 7 days on potassium chloride. They don’t seem to report a test against baseline but it probably would not be significant because the sample size was only 14.]
These Slow-K tablets themselves are just over 300 mg potassium in a “sugar-coated (not enteric-coated) tablet”. Taking 12 of them a day for a week seems to work out just fine.
In this chronic kidney disease study from 2022, participants were given a daily dose of about 1,500 mg potassium in “two capsules, three times per day during meals”. This presumably works out to a total of six capsules a day, or about 250 mg potassium per capsule. In this group with chronic kidney disease, 11% (mostly the older participants) did develop hyperkalemia. But no one developed small-bowel lesions.
We could keep going like this for a while — many studies give people several thousand milligrams of KCl per day, in forms that contain well over 100 mg of potassium per tablet. As long as tablets aren’t enteric-coated, and people don’t have chronic kidney disease, this turns out just fine. KCl by itself at reasonable doses is quite safe. You can literally buy sacks or jugs of potassium chloride on Amazon, mostly for use in electrolyte solutions (i.e. make your own Gatorade).
Study Design
The design of the study is simple: supplement low doses of potassium directly, and see if people lose weight. Super easy, low cost. And you’re probably not getting enough potassium to begin with.
This design is similar to the design we used for the potato diet. The main difference is that you will be chugging potassium salt solution instead of eating potatoes, and you can keep eating normal food like usual.
This study will run the same length as the potato diet so that the two can be compared directly — 28 days, with the final weight measurement on the morning of day 29. But we encourage people who are having a good time with the potassium to keep going and report back again at 60 days.

Supplemental Potassium
We recommend that you use Nu-Salt as the source of your potassium chloride, because that is what we tried and it worked for us. All terms and measurements below will be in Nu-Salt terms; if you use something else, make sure to convert all units to whatever form of potassium you are eating.
You can buy 3 oz shakers of Nu-Salt in various places, including on Amazon. A 3-pak should be enough to cover 28 days of potassium supplementation for most people, but if you want to share with your friends and family, or you’re confident you want to supplement potassium for longer, you can also buy a 12-pak.
There are many other potassium chloride brands you could try if you want, like this Morton salt substitute (though we tried this one and found it to be *extra* gross). You could also try another potassium compound, like potassium citrate. We would prefer that most of you stick to KCl, but if a few of you tried other compounds that might be interesting, in case they end up being clearly much more or much less effective.
We’re asking participants to buy their own potassium, and we feel ok about this because potassium salt is pretty cheap, only about 80 cents per ounce. As of this writing, the 3-pak of Nu-Salt Shakers (totaling 9 oz of KCl) is only $7.48 on Amazon. But if you want to participate in this study and you really can’t afford it, contact us and we’ll send you some.
How to Consume
Potassium chloride by itself tastes pretty gross to most people, bitter and metallic all at the same time. This gang of Australian teens tasted all the alkali metal salts, and if you can get past their literally nauseating camerawork, you’ll see that they describe potassium chloride as “really bad” and “weird” and “cold on my tongue” and “it tastes like how bleach smells” and “oh god, what is it?” They still gave it a 3/10 though, which is a higher rating than they gave cesium chloride.
The good news is that it doesn’t take much to mask this unpleasant taste. If you mix the potassium salt into food or beverage, it becomes much easier to handle.
We fooled around with a few approaches, but ultimately we found that it’s easiest to just dissolve the KCl in a glass of water, or Gatorade / Powerade / Vitamin Water. Often we did potassium in a mixture of half water and half one of these drinks. The flavor of 1/8 tsp KCl in a 20 oz drink is pretty understated — the water just feels “smoother”, almost like a fancy mineral water. Which it kind of is.
You can improve the taste a little more if you also add a bit of table salt (NaCl). We found that a mix of 2:1 KCl to NaCl tastes pretty ok — not too salty and not too metallic. For example, if you were putting 1/4 tsp KCl in a Gatorade, adding 1/8 tsp NaCl is a good idea to keep the potassium taste from being overwhelming. But some electrolyte powders contain higher ratios and may be more effective/taste better, so feel free to experiment with adding more (or less) NaCl.
Adding lemon juice or sugar can also help offset the taste. As you can imagine, if you take this line of thinking to its natural conclusion you’ll end up drinking slightly salty lemonade. It’s not too bad.
We also sometimes tried putting the KCl in food. You can hide small doses in flavorful foods like beans, or in sauces, but if you overshoot at all, the food ends up tasting pretty weird.
Our most successful food discovery is that KCl goes really well with mustard. You can mix 1/4 teaspoon into a generous helping of mustard and barely taste it at all. If anything, KCl gives the mustard a tingly, almost effervescent feel.
If we were normal influencers, this is where we would start promoting DR MOLD-TIME’s KALIATED WEIGHT LOSS MUSTARD. Sadly we don’t know how to sell condiments, but hit us up if you want to do a partnership.
Dosing
How to Supplement:
- Take at least one dose per day.
- But no more than 4 doses per day.
- Always take doses at least an hour apart.
- Take doses with plenty of water. It’s also recommended you take them with some table salt, or eat something salty right after.
- We recommend that each dose be at least 330 mg potassium (1/8 tsp Nu-Salt).
- However, never take more than 1300 mg potassium (1/2 tsp Nu-Salt) in a single dose.
- This means the maximum daily dose from KCl supplementation is 5200 mg, which is high but still less than you would get on the potato diet.
- If you have to miss a few days that’s fine, just pick it back up when you can.
In the grand scheme of things, these are pretty low doses. A few hundred milligrams of potassium isn’t much, and this dosing scheme will never give you anywhere near the amounts of potassium people were getting on the potato diet.
If this setup doesn’t cause weight loss, it’s still possible that potassium could be the active ingredient in the potato diet, and the dose on this protocol is simply too low to budge your lipostat. But, safety first, and we hold out hope that small doses may have clear effects, even if the effect of this study is smaller than the potato diet.
Protocol
Now that we’ve established these basics, here’s the study protocol:
- Start with two doses of 330 mg potassium (1/8 tsp Nu-Salt) on the first day.
- If you feel fine, try three or four doses of 330 mg potassium (1/8 tsp Nu-Salt) on subsequent days.
- If you’re feeling fine after 4-7 days, try one dose of 660 mg potassium (1/4 tsp Nu-Salt).
- If you still feel good, keep increasing your dose by small increments. For example, if you are on two doses of 660 mg (1/4 tsp Nu-Salt) a day, you might increase that to three doses of 660 mg, or one dose of 660 mg and one dose of 1300 mg (1/2 tsp Nu-Salt). If a higher dose makes you feel bad, try returning to the dose you were on before and maintain that.
- Try slowly increasing to two doses of 1300 mg (1/2 tsp Nu-Salt) a day. Only go beyond that if you are feeling totally fine.
- You should calibrate based on your own experience — different people will have different needs and different limits. For example, we’d expect someone who weighs 300 pounds would be able to tolerate higher doses than someone who weighs 150 pounds.
- If you feel weird / bad / tired / brainfog and you can’t tell why, try:
- eating something;
- drinking some water;
- getting some sodium;
- and see if any of those help. It may be easy to end up needing food / water / salt and not notice.
- If you still feel weird, try dropping to a lower dose or taking 1-2 days off.
- If at any point you feel sick or have symptoms of hyperkalemia (see below), stop immediately and seek medical attention.
This is not a diet. You should continue eating as normal, and food should mostly be consumed ad libitum (eat as much as you want). But there’s one important guideline we want to note. Because potassium supplementation seems like it strongly reduces appetite in some people, you may actually need to eat more than you feel like. We strongly encourage you to make sure you get at least 1000 calories a day, preferably more.
It’s fine to take breaks in the middle or even stop the trial early. But if you sign up, please record 4 weeks of data even if you stop taking potassium at some point, have to end early, have to take a break in the middle, or can’t stand taking KCl for the full 4 weeks. If you do it for two days and hate it, please keep recording your weight and potassium consumption (which would just be zero from then on) for the full 29 days and submit your data as normal. We can still use it!
Our hope is that this will keep us from running into the dropout issues we had in the potato diet. Anyone who records data for 29 days is clearly taking the study seriously, even if they weren’t able to stick to the potassium supplements the whole time.
Based on this, our main analysis will focus on participants who provide 4 weeks of data. If you provide a weight measurement for the morning of day 1 and the morning of day 29, so we can calculate your weight before and after, and you took at least one dose of potassium, we will do our best to include you in the analysis.
Variables
Speaking of which, here are the variables we want you to track.
The main outcome of interest is your weight, taken every morning, after your first “void”, assuming you void in the morning.
We also want you to track your potassium supplementation. We’ve provided four fields per day for potassium doses and notes, since we ask that you take no more than four doses per day.
There’s a possibility that potassium causes weight loss by protecting you from lithium, and there’s a chance that certain foods are especially high in lithium. We aren’t confident enough about this to ask you to avoid these foods, but we do want to ask you to track how much you’re eating them. We’ve provided fields for meat, eggs, dairy, leafy greens, and tomato products, all of which are currently top lithium candidates. If you eat more than a smidge (by your own judgment) of any of these foods, please put a “1” in that field for that day. If not, put a “0”.
This way, we can see if any of these foods seem to inhibit potassium weight loss. Relatedly, if you’re supplementing potassium and not seeing any weight loss, you could always try cutting back on the cream and ketchup.
We’ve also included fields for several BONUS VARIABLES. You don’t have to track these, but if you do, the standardized fields will let us analyze these results across participants. In particular, we’d be interested in having data for your blood pressure, sodium intake, and energy/mood, but we’ve included several more fields for variables people might want to track. There’s also a field for tracking waist circumference, which a couple people asked for after the potato diet.
We also included fields for up to 10 extra variables of your choosing. If you want to record anything else, please put it here. This way you can add more variables without changing the format of the data sheet, which would make it harder to analyze your data. So please don’t touch the formatting, but feel free to add variables in the extra variables area.
And speaking of other variables — Michael Dubrovsky of SiPhox reached out to us to offer a discount to participants who want to test their blood biomarkers with SiPhox’s at-home Quantify kits. We haven’t had a chance to try these kits, but if you’re interested check it out. You can get a two-kit bundle (so you can do one test before the trial and one after) for 40% off at this link.
That’s the gist. Before you sign up, however, we insist you read this section on safety:
Safety
Do not participate if you have diabetes or any kind of impaired kidney function.
For everyone else, this level of potassium supplementation should be very safe.
Until recently, it was recommended that adults get 4,700 mg of potassium per day in their diet. Most people seem to get less than this, so supplementing is probably a good idea anyways.
Going over 4,700 mg of potassium a day is also very safe. Most people in the NHANES data got less than the recommended amount, but a small number were estimated to get over 10,000 mg in their diet. The potato diet also seems to indicate that you can take a lot of potassium and not get sick. As a reminder, 2000 calories of potatoes gives you more than 10,000 mg of potassium.
In addition to recommended allowances, the National Academy of Medicine also sets tolerable upper intake levels (ULs) for vitamins and minerals. But normal doses of dietary potassium are so safe that no upper level has been set, for lack of information. This chapter from the National Academy says, “Although dietary potassium intake can be increased through behavioral change, there is a self-limiting aspect to such changes that makes toxic adverse effects from increases in dietary potassium intake unlikely.”
This study focuses on potassium chloride specifically, which is quite safe. It’s sold as a salt substitute and electrolyte powder — you can buy it in bulk on Amazon. Studies of hypertension sometimes prescribe as much as 3,700 mg potassium a day as potassium chloride, without any apparent ill effects.
The toxicity of potassium chloride is low. The LD50 for potassium chloride taken orally is around 2,500 mg per kilogram of bodyweight. If you weigh 165 lbs, you would start to be in danger at doses of around 190,000 mg.
Like any substance, very large doses can be dangerous. The main danger is unsurprising — hyperkalemia, which is the condition of having too much potassium in your blood. But to get there, you have to A) take a lot of potassium, B) have kidney problems, or C) both.
The National Academy summarizes the few case studies that are known. The first is from 1978, a 32-year-old woman who died after ingesting an estimated 47 extended-release potassium chloride tablets.
The second is from 2014, a report of a 26-year-old man who died after consuming an estimated 12,500 mg of potassium, in the form of extended-release potassium chloride tablets. However, “there was also co-ingestion of dextropropoxyphene-acetaminophen in this case, which complicates the interpretation.”
These are the only deaths they report (“death is a particularly severe endpoint to use to establish a UL”), but they review two other case studies as well. One is a case report of a 17-year-old man who developed nausea, vomiting, and diarrhea after consuming around 10,000 mg of potassium as sustained-release potassium chloride tablets.
Another describes a 67-year-old man with kidney injury who had a heart attack after consuming around 2,730 mg per day of potassium from a salt substitute for one week. He also “reportedly consumed a high-potassium diet, in addition to the salt substitute.” They note that, “the amount reportedly consumed from the salt substitute is a level of intake that has been repeatedly studied in potassium supplement trials, wherein the risk of adverse events appears to be low among generally healthy populations.” We agree — 2,730 mg per day seems very safe if you are not a 67-year-old man with a kidney injury.
The worst-case scenario in this study is that you develop hyperkalemia. If you have healthy kidneys, this shouldn’t happen. But just in case, here are the signs and symptoms.
Symptoms of mild hyperkalemia include muscle weakness, numbness, tingling, and nausea. These could also indicate that you’re not getting enough food, water, or sodium. If you start feeling these symptoms, try eating, drinking some water, or having some table salt or salty food. If the symptoms persist or get worse, consider ending the study or at least taking a break.
Symptoms of severe hyperkalemia include abnormal heart rhythm, heart palpitations, shortness of breath, chest pain, sudden nausea, and vomiting. If you have any of these symptoms, end the study immediately and seek medical attention. If you have an existing reason you might experience one of these symptoms (you already sometimes have heart palpitations or get nauseous suddenly), do not sign up for this study, since if you had symptoms of hyperkalemia, you wouldn’t be able to tell.
Sign Up
Ok, now you can sign up.
The only prerequisites for signing up are:
- You must be 18 or older;
- In generally good health and specifically with no kidney problems;
- Willing to supplement potassium, as described above, for at least four weeks, and;
- Willing to share your data with us.
Also, we’d prefer that you don’t sign up for this study if you were already a participant in the potato diet study. We’d love to have your help again, it’s just that if you lose even more weight on potassium, that will mess up the 6-month weight-loss followup numbers for the potato diet. Those of you who have tried the potato diet but weren’t officially part of our study can still sign up.
As usual, you can sign up to lose weight, lower your blood pressure, get more energy, or see one of the other potential effects. But you can also sign up to help advance the state of nutritional science. This study will tell us something about nutrition, by either supporting the idea that potassium is the reason the potato diet causes weight loss, or providing evidence against it.
Beyond that, running a study like this through volunteers on the internet is a small step towards making science faster, smarter, and more democratic. As always, that seems like a future worth dreaming of, and if you sign up, you get us closer to that future.
Potassium salt is a little gross, so you might be wondering if you really want to commit to this for several weeks. But here’s our suggestion: If you are at all interested in trying it, go ahead and sign up and start collecting your data. Try the first day or two and see how it feels. If you hate it and have to stop, we would still love to have that data.
If you want to go for longer than four weeks, that’s great, we would be happy to have more data. Report your data at four weeks like normal and then just keep going, and if you make it to 60 days, send us an update.
If at any point you get sick or begin having side-effects, stop the diet immediately. We can still use your data up to that point, and we don’t want anything to happen to you.
We are mostly interested in weight loss effects for people who are overweight (BMI 25+) or obese (BMI 30+), but if you are “normal weight” (BMI 20-25) you can also sign up. The potato diet caused weight loss in people of normal weight, and it would be interesting to see if the same thing happens here.
And for everyone, please consult with your doctor before trying this or any other weight loss regimen.
Anyways, to sign up:
Fill out this google form, where you give us your basic demographics and contact info. You will assign yourself a subject number, which will keep your data anonymous in the future.[UPDATE: Signups are now closed, but we plan to do more studies in the future. If you’re interested in participating in a future study, you can give us your email at this link and we’ll let you know when we run the next study.]- We will clone a version of this google sheet and share the clone with you. This will be your personal spreadsheet for recording your data over the course of the diet.
- On the first day, weigh yourself in the morning. If you’re a “morning pooper”, measure yourself “after your first void”; if not, don’t worry about it. We don’t care if you wear pajamas or what, just keep it consistent. Note down your weight and the other measures (mood, energy, etc.) on the google sheet. Start with two doses of 330 mg potassium (1/8 tsp Nu-Salt) on the first day. On day 2, weigh yourself in the morning, note down data in the sheet, then take at least two doses of 330 mg potassium (1/8 tsp Nu-Salt). On day 3, etc. See the dosing protocol above for details.
- We prefer that you keep taking at least one dose of potassium a day for at least four weeks. But if you do have to miss some days, or need to take a break, just note that down and keep recording other variables. If you totally can’t stand the potassium, just stop taking it, keep recording other variables until day 29, and submit your data as normal, we can still use it.
- When you reach four weeks, and take your weight measurement on the morning of day 29, send us an email with the subject line “[SUBJECT ID] Potassium Trial Complete”. This will let us know to go grab your data. This is also your opportunity to tell us all about how the study went for you. Please tell us any data that doesn’t easily fit into the spreadsheet — how you felt, what kind of potassium you used, before and after pictures (if you want), advice to other people trying this, etc.
- You may reach day 29 and decide to keep going longer. That’s fine. Send us an email on day 29, and if you reach 60 days, send us another email and we will grab your data again. If we get enough data we might do an analysis of this longer span as well. If you go past 60 days and want to share it with us at some point, that’s cool too.
- If we have our act together, we will send each of you a brief google form following up at future points.
Assuming we get 20 or so people, we will write up our results and publish them on the blog. We would really like to get a couple hundred people, though, since at that point it becomes possible to do more complex statistical analyses. So if you think this is an interesting idea, please tell your friends!
Special thanks to Austin Vernon for helping us automate parts of the signup process.

Man, this looks very exciting. I’ll stay out for now because I am both still on a long-term keto project (since 2021) that’s very effective, and the confirmed continuous losses from that would confuse results of the experiments I think.
And because I’m even less sure if the Kalium Chloride they’re selling here is even in the right amounts etc. for the experiment. I think potential users of metric would be very thankful if you had that as an alternate unit 😀
LikeLiked by 1 person
Shouldn’t you do a study on people using water filters that remove lithium, to see if it lowers body weight?
One of the main hypothesis of the blog is that lithium is causing the world wide obesity epidemic. An earlier post showed which water filters removed lithium. If you have people only drink and cook with the filters that work, you should be able to quickly prove or disprove the hypothesis. That could be big.
LikeLike
Possibly — we need to figure out how much lithium is in food first, since if there is 100x more lithium in food than in water, then water filters won’t do much. So we’re holding off on a water filter study until we can test some food samples, then we’ll revisit the idea.
LikeLike
I’d like to try this with tablets — experience teaches that I’ll take any amount of pills but I won’t drink weird-tasting stuff. Should I sign up? I don’t want to mess up your data, but I think I’ll give it a try in any case.
LikeLike
I’d like to try it but with 99mg tablets, should I sign up or will that just mess up your data? Experience teaches that while I’ll take any amount of pills, I won’t drink weird-tasting stuff on the regular.
LikeLike
Sure, any kind of food-grade potassium works for us, just note it down!
LikeLike
I’m currently trying the potatoe diet and realized how difficult is to even get my recommended 2000 kcalories just by eating potatoes. I’m not sure if you have ever eaten 2kg of potatoes, but it is a lot, and certainly more food than I would consume on a regular week!
How can you be sure that the potatoe diet is really doing something different than CICO (and has anything to do at all with potassium) if you haven’t controlled for actual food intake?
LikeLike
The Nu-Salt/salt combination drink you’ve described is basically “snake juice”, which is often used to replenish electrolytes in fasting.
https://www.reddit.com/r/fasting/wiki/fasting_in_a_nutshell/you_need_electrolytes
You can probably find recipes for more palatable versions in that community.
There’s apparently also a commercialized fad diet version:
https://www.reddit.com/r/snakejuice/
It’ll be interesting to see how important the fasting part actually is.
Also, someone suggested you can get potassium tablets >99MG outside of America. Seems to be true:
LikeLike
Yeah, for additional reference, the electrolytes that I use while fasting have 500mg potassium per serving: https://www.ketovitals.com/products/berry-anti-oxidant-electrolyte-powder-tub-strawberry?variant=39340061458474
LikeLike
Is chicken “meat” for tracking purposes? I would assume that it is, just checking.
LikeLike
Yes, it is
LikeLike
Do you have any thoughts on the possibility vitamin B6 causes obesity?
In the 2019 paper you cite (https://www.mdpi.com/2072-6643/11/6/1256/htm) it has a very strong positive effect on obesity (stronger than total calories or sugar intake).
It caught my eye earlier (I think you cite it in a potato post as well) after having seen this blog post https://medium.com/@rnikoley/how-food-enrichment-promotes-obesity-275989cb03b7 maing the case that B6 supplementation/enrichment in the US has caused some obesity. The post i a bit bombastic, but the old ads about yeast for weight gain are super interesting.
Really enjoy your work, curious about your thoughts on this!
LikeLike
Do you have any thoughts on the possibility vitamin B6 causes obesity?
In the [2019 paper you cite](https://www.mdpi.com/2072-6643/11/6/1256/htm) it has a very strong positive effect on obesity (stronger than total calories or sugar intake).
It caught my eye earlier (I think you cite it in a potato post as well) after having seen [this blog post](https://medium.com/@rnikoley/how-food-enrichment-promotes-obesity-275989cb03b7) making the case that B6 supplementation/enrichment in the US has caused some obesity. The post i a bit bombastic, but the old ads about yeast for weight gain are super interesting.
Really enjoy your work, curious about your thoughts on this!
(this is a test comment. I posted the same thing a minute ago but accidentally way less anonymously ¯\_(ツ)_/¯ ) (would prefer this one)
LikeLike
We’re generally skeptical of vitamin theories but there are a few data points we’ve recently come across that make them seem more interesting (though weirdly the evidence maybe points to different vitamins?). This is something we might revisit — the potato diet certainly does keep you away from all fortified foods, that’s a plausible mechanism.
LikeLike
Can you give a suggestions of products available in the UK and Europe. Nu Salt is around $150 for a 12 pak on Amazon UK. Pure KCL powder or 1000mg potassium citrate tablets are easily and cheaply available. In stores, a product called “Lo Salt” is available which has “66% leess sodium” so that might be 2/3 KCl to 1/3 NaCl which would be close to your suggestion here. (Says 450mg potassium, 430mg salt in a 1/4 teaspoon).
LikeLike
If you can’t get Nu-Salt, any food-grade potassium salt or potassium supplement can be substituted, just make sure to do the calculations so you’re getting the right amount (e.g. starting with two doses of about 330mg) and note down what kind of potassium you’re using so we can see if the source makes a difference
LikeLike
Interesting, but as someone with heart issues, this isn’t the study for me! 🙂
Indeed, I wonder if the potato diet would be dangerous for people with heart issues, too?
LikeLike
Are you aware of Marty Kendall’s work on nutrient density and satiety? This blog post claims that (based on thousands of days worth of food logging from users of the site) people consume fewer calories on days they consume more potassium. Other minerals also have effects but potassium is strongest.
https://optimisingnutrition.com/minerals-hunger-and-satiety/
LikeLike
No but that’s very interesting, thank you for the pointer!
LikeLike
My math might be wrong here (or I might be looking at a different formula of Nu-Salt?), but I think your Nu-Salt conversions are off here. According to the nutrition facts on Amazon, one serving is 1/6 tsp, which has 530mg of potassium; 1/8 tsp is 75% of 1/6 tsp, and 75% of 530mg is 397.5mg, not 330mg. Obviously 67.5mg isn’t that much, and even the highest intake of two 1/2 tsps per day is only 580mg difference, but I just wanted to make sure I wasn’t reading anything incorrectly.
LikeLike
Yes, we’ve seen several different labels for Nu-Salt and they don’t always agree exactly, we’re not sure what’s going on there. They may have changed the label recently? All the measurements are in the same ballpark so it’s good enough for the first study, where we’re just trying to get a rough estimate of the effect size (if any).
LikeLike
I assume some people in the study have a scale that can measure on the gram scale relatively accurately. If that’s the case (and assuming Nu-Salt is pure KCl) potassium is 52.45% of the weight.
LikeLike
I am in the UK and Nu Salt is expensive at around £15 for 3oz, so I opted for BonSalt (from Spain) at less than £12 for 3 x 85g tubs. It is 0.45g in 1g so I just add it in to my coffee in the morning. I use the Nespresso into the mug, place the mug onto the scale and weigh 1g. The tubs have fused lids so I can’t take them off to measure with a spoon, but this way is no problem and more accurate.
LikeLike
Inspired by the parent comment, I checked the label on the Nu-Salt I bought for this study, and tried to determine the math on my own. (Mostly, I was unable to determine on my own what percentage the potassium would be by weight. (It has just occurred to me that it’s the ratio of the atomic weights involved and this matches ijusteatit’s number, hooray.))
My Nu-Salt says, relevantly: 1/4 tsp (1.25g), Potas. (15% DV). No remark about milligrams of potassium, but 1/8 tsp does correspond to 328 mg potassium, assuming it’s pure KCl. Mostly, I find it interesting that the implicit Daily Value is 4370 mg of potassium. This led me to here: https://ods.od.nih.gov/factsheets/Potassium-HealthProfessional/ which, in the paragraph under Table 2, does claim that the DV for potassium is still 4,700 mg, while the Adequate Intake value is lower (as mentioned in the blog post).
This comment started as an attempt to document and double-check some math and has ended up on “it looks like everything is fine here”. Still need to experiment with ratios, dilution, other flavorings, to see what’ll make this stuff palatable.
LikeLike
The Nu-Salt label says: “1/6 tsp (1 g) is 1 serving; 530 mg potassium per serving.” This looks right since potassium chloride is ~53% potassium. So your dose of 1/8 tsp (0.75 g) will be 397.5 mg, not the indicated “330 mg”, per multiple. Or is another factor in play?
LikeLike
Very interested and enthusiastic for this citizen-science approach. Did you consider asking participants to log weight for a week or so before starting potassium (or even starting to log, then cueing them to start taking potassium some random number of days between 7-14 after starting). This might control for confounds, like mindfulness of weight and eating when you start recording weight every day etc.
LikeLike
I got my Nu-Salt in the mail today and am hoping to start tomorrow. I submitted my google form at least 24 hours ago, when should I expect my spreadsheet link? I can clone the one you have, but sounds like you want to have one to share to us.
LikeLike
You should have it by now but it’s possible we made a mistake. Send us an email with your participant ID number?
LikeLike
Hi, why does it say below 330 is 1/8 tsp? The Nu Salt shaker says 1/4 tsp is 1.25 g.
LikeLike
1/4 tsp is 1.25 g of potassium chloride, but that’s the compound. The potassium in that compound weighs a fraction of the total compound.
LikeLike
I guess it shouldn’t be surprising that many foods widely regarded as “health” foods are actually very high in potassium…
LikeLike
I searched for a minute or two and found a potassium supplementation RCT that measured body weight changes: https://pubmed.ncbi.nlm.nih.gov/11446724/
The experimental group participants had 2.3 additional grams of potassium per day, for 12 weeks, and experienced no change in body weight.
LikeLiked by 1 person
That’s a comparatively small study of only 150 people, with a baseline BMI that looks like “overweight” rather than “obese”, and the pdf explicitly states that “Participants met with a dietician regularly to monitor their diet in order to keep body weight constant during intervention” so I’m not sure it is very conclusive!
LikeLike
That is not the only study.
In the hypertension study from 1985 linked in the post, there does not seem to be a change in body weight.
This other RCT https://www.cambridge.org/core/services/aop-cambridge-core/content/view/BAD451CD40EEC5B843ED671D6E323C4F/S0007114503002435a.pdf/the-effect-of-low-dose-potassium-supplementation-on-blood-pressure-in-apparently-healthy-volunteers.pdf likewise finds no change in body weight (after 6 weeks of 1 g/day potassium supplementation).
This meta-analysis https://pubmed.ncbi.nlm.nih.gov/12821954/ finds a median loss of 0.2 kilograms after a median of 6 weeks across several RCTs of potassium supplementation, but more than double that loss after a median of 4 weeks in sodium restriction RCTs
LikeLiked by 1 person
I bought a saltshaker of the brand ‘lo salt’ to participate in this study which contains 33% NaCl and 66% KCl. To compare it to the doses you are recommending I was making a conversion table, but it seems that you have used a much higher gram per teaspoon?
The (dutch) source I found counts 2 gram salt per teaspoon (https://www.voedingscentrum.nl/nl/gezonde-recepten/kookhulp/hoeveel-gram-milliliter-theelepel-eetlepel.aspx, voedingcentrum is the dutch
government subsidized institution for nutritional advice). Guessing from the mg potassium doses you are giving here I think you have used between 5 and 6 gram salt per teaspoon?
Would be helpful if you added the amount of grams as well in the study design and/or the instructions in the spreadsheet!
LikeLike
Hello! I forgot to record my ID number, and I did get the spreadsheet shared with me. Should I reapply with a new number or should I do something else? Thanks.
LikeLike
Your ID number should be on the spreadsheet? Email us if you have more questions about this. 🙂
LikeLike
FWIW, the Wikipedia article about potassium says (though without any citation): “Potassium is also available in tablets or capsules, which are formulated to allow potassium to leach slowly out of a matrix, since very high concentrations of potassium ion that occur adjacent to a solid tablet can injure the gastric or intestinal mucosa. For this reason, non-prescription potassium pills are limited by law in the US to a maximum of 99 mg of potassium.”
Despite the lack of a supporting citation, that does seem physically plausible as a reason to limit the concentration of solid pills. But it also sounds like it isn’t a direct concern for the dosing protocol described in this post, which involves diluting the salt in comparatively large volumes of water before ingestion.
LikeLike
So, different countries have different formulations of Nu-Salt? Do you have people include the manufacturer’s lot number in the spreadsheet?
LikeLike
A handy calculator for weights and volumes of NuSalt: https://www.aqua-calc.com/calculate/food-volume-to-weight/substance/salt-blank-substitute-coma-and-blank-upc-column–blank-04482238
LikeLike
Potentially it would be easier to suggest people create a KCl solution for dosing purposes? I say this as someone lacking a 1/8 teaspoon in the drawer.
3 oz NuSalt container = 84.9g
84.9g KCl = 44.5g K
Dissolve entire container into 4000 mL of water
500 mg K = 45mL (same as shot of alcohol)
If lacking a 4L carboy, dissolve 21.2g NuSalt (84.9g / 4) into 1L bottle.
LikeLike
Wondering if anyone has been dealing with slight stomach discomfort — cramps, gas? Taking 3x/day 1000mg doses of potassium chloride — https://www.fahorro.com/kaliolite-500mg-oral-50-tabletas.html (2 tablets/dose)
LikeLike
I have some gas but it is less than on the 1st day when I felt I was being purged multiple times in the day. That settled on day 2.
I’m on day 4 and I have had 2 x 900mg in coffee/water. I plan to have another 2 doses today.
One thing though, last night I woke at 3 am and didn’t get back to sleep for well over an hour. I kept thinking about work, even though it is my day off. I feel a bit down today as well. Hopefully, that is temporary as KCL should resolve that and I don’t usually have these issues.
LikeLike
I also found myself waking up in the middle of the night for the first few days, but it seems back to normal after a few days. I intentionally don’t take any potassium at night now though.
LikeLiked by 1 person
Anyone else tried crushing tablets? Read into the enteric coating issue but think the tablets I’m getting here are probably the best deal (and easiest dosage): https://www.fahorro.com/kaliolite-500mg-oral-50-tabletas.html — did get a bit of stomach unease w/o crushing first 2 days.
LikeLike
Thoughts on mixing Nu Salt with an electrolyte powder like Liquid IV or Pedialyte?
LikeLike
Sure, just be aware that those will contribute some potassium as well, so mind the overall dose!
LikeLike
I found that 1/4 tsp nu-salt + one packet of liquid IV actually tastes good in my opinion. My favorite is the tangerine flavor.
LikeLiked by 1 person
(with around a liter of water, like usual with liquid IV)
LikeLiked by 1 person
A liter! I’ll try that for my next dose, I haven’t been having the greatest time with 12-16oz. Thanks!
LikeLiked by 1 person
I am a Type 1 Diabetic who has been following your work for some time. I am extremely compelled by your entire body of work and I’m particularly interested in the idea of potassium supplementation. I know there have been some links shown between low levels of potassium leading to lower levels of insulin production (and has been particularly associated with Type 2 diabetes), but as a Type 1 who relies on manual injections of insulin, I have to wonder if low levels of potassium supplementation would be safe and provide some similar results.
I’m going to follow-up with my endocrinologist but can you clarify what specific risks you’re concerned about for diabetics? Is it the increased risk to kidney function for poorly controlled diabetics? I’d love to hear your thoughts — to clarify, not planning to enter any of your community trials for fear of complicating results but interested for my own (possible) experimentation.
LikeLiked by 1 person
Yes, we’re primarily concerned about kidney function and the resulting risk of hyperkalemia. But just in general, we don’t know if there are any benefits of potassium at these doses, we know there maybe be minor risks for some people, so we figure let’s let people who are as healthy as possible test this first. We’ll have results in a couple of weeks, and if we find there’s any benefit, then everyone can start thinking about the risk-benefit calculation for themselves.
LikeLike
Appreciate the response, makes sense
Also, yes agree about potassium >> insulin but not too optimistic
LikeLike
That’d be super interesting if taking potassium resulted in insulin production.
LikeLike
Is tuna or other fish meat for the purposes of tracking?
LikeLike
Yes
LikeLike
I just found out that (at least some brands of) coconut water have quite a lot of potassium. Is there any reason to beleive that chugging that would be significantly less likely to act as a bolus dose compared to, for example, NuSalt disssolved in Gatorade?
LikeLike
We really don’t know, so it seems like it’s worth it if some people give it a try.
LikeLike
I just returned to this website last week to see if there were any new developments on a “chemical hunger” so I am late to this study, but I wanted to report that after reading it I bought this supplement: https://shop.drberg.com/electrolyte-powder-raspberry-lemon-100-servings
I realize it is potassium citrate instead of chloride, but this stuff tastes great. I swim long distance and occasionally get cramps so after reading this, I knew I wasn’t getting enough potassium.
LikeLike
Did you get the 20 participants? When will you publish?
LikeLike
We did! Check our archives. it was published on 12/20/22
LikeLike