Single-subject or single-case research designs date back to at least the 1980s — though as you can see from the sparse Wikipedia page, they haven’t gotten that much attention. While the idea of single-subject research is good, the execution tends to be crap.
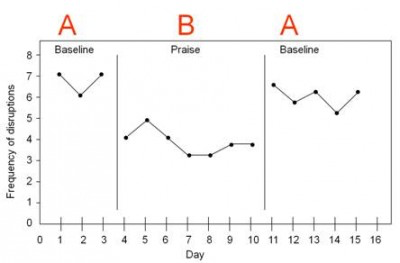
The simplest single-subject design is the “ABA” design, where you have a few control days (“A”), a few days on the treatment (“B”), and then you go back to the control (“A”). See for example this figure from the University of Connecticut:
In this case, we can see that “frequency of disruptions” (from a target student) is high in the first baseline A block, goes down for a while in the B block (“praise”), and goes back up when they switch back to A.
The ABA design is better than nothing. It’s better than a case study, because at least there’s some experimental control. But it just doesn’t give us all that much information. They have 15 days of data, sure, but only three phases. This is really more like a sample size of three (not that a sample size of 15 is all that much more compelling).
Some sources might recommend the more advanced ABAB approach…
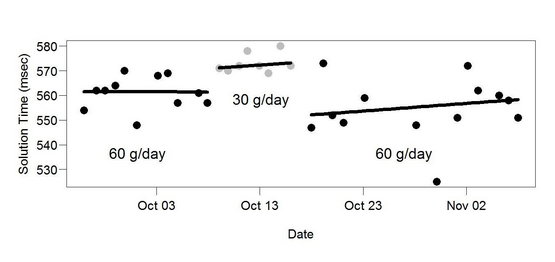
…but ABAB isn’t all that convincing either. Is that a change in the periods of “positive attention”, or just a random walk? It’s pretty hard to tell.
Again, this is vague at best. Yes, it took him longer to do arithmetic problems on 30 g/day butter than on 60 g/day butter. But the change is not very distinct, the three periods clearly overlap, it’s not clear if the periods were randomly determined, etc. And most of all, the sample size is just not very large — we can do better than drawing strong conclusions from a mere three intervals.
You shouldn’t totally discount these simple designs. Starting here can be fine (see for example Allan Neuringer’s self-experiments). Simplicity is important, and if you’re doing early stage exploratory work, going with a study design that’s easy has obvious benefits. If you don’t see any difference with this simple approach, you can move on to something else. If you do see a difference in the ABA, and you want to demonstrate that difference in a more convincing way, then you can expand it into a true within-subjects study.
There’s nothing wrong with Seth’s butter ABA — it’s just that it looks like the start of something, rather than a conclusion. If he wanted to really convince people, he should have spun that off into a longer self-experiment.
Within-Subjects Approach
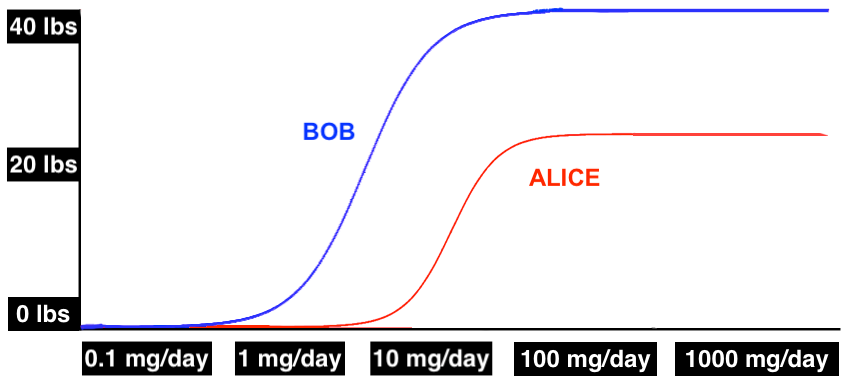
Emily is a woman in her late 20s who gets migraines on a regular basis. She usually gets hit with a migraine in the middle of the afternoon, and they happen almost every day. Emily has been tracking her migraines for a long time, and has determined that each day there’s an 80% chance that a migraine will descend on her at about 2:00 pm, ruining the rest of her afternoon.
Emily has recently noticed that if she takes 400 mg magnesium in the morning, it’s much less likely she’ll have a migraine that afternoon. This isn’t a sure thing — she still gets migraines on days when she takes the magnesium — but it seems like it’s less than 80%.
One way for Emily to get some support for this hypothesis would be for her to run a simple AB self-experiment. She could take no magnesium for two weeks, then take 400 mg magnesium every morning for two weeks, and see if it makes a difference for her migraines. If she gets migraines 80% of the time in weeks where she’s taking no magnesium and only 40% of the time in weeks where she’s taking 400 mg magnesium, that seems like evidence that the magnesium is helping.
And it is evidence, but it’s on the weak side. Depending on how you slice it, the effective sample size here is two — just one fortnight with magnesium, and one fortnight without. You shouldn’t draw strong conclusions here for the same reason that you shouldn’t draw strong conclusions from a study with one person in the experimental group and one person in the control group. There’s just not that much evidence.
With small sample sizes, there are too many alternative explanations, it’s too easy to fool yourself. Maybe she started taking magnesium in the springtime, and the increased daylight is the real reason her migraines improved. Or she just started a new job two months ago, and it took her two months to stop grinding her teeth, which happened to align with the switch over to magnesium. Or her detergent manufacturer switched to a new supplier for fragrances. Or maybe her mailman’s cat, which she’s allergic to, ran away last week. It could be almost anything.
To account for these problems, Emily can just go ahead and get a larger sample size. She can use a random number generator to randomly assign days to either take magnesium or not take magnesium, and then follow that random assignment.
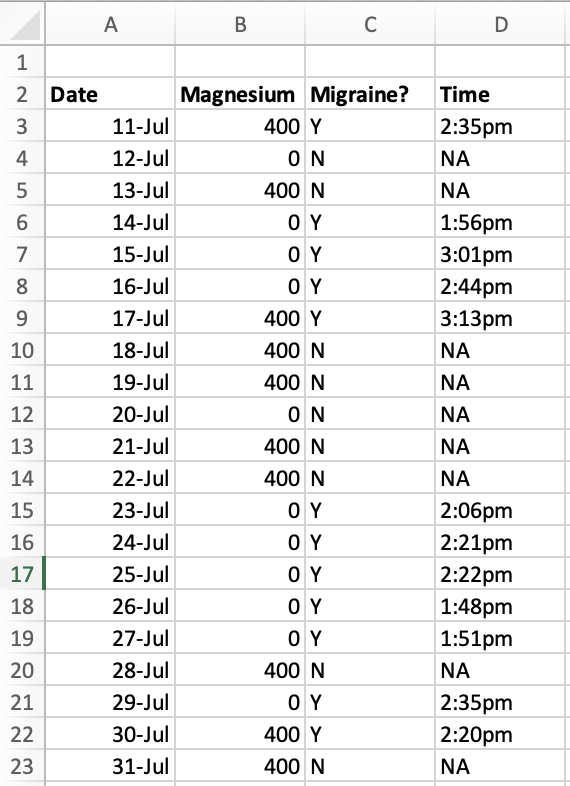
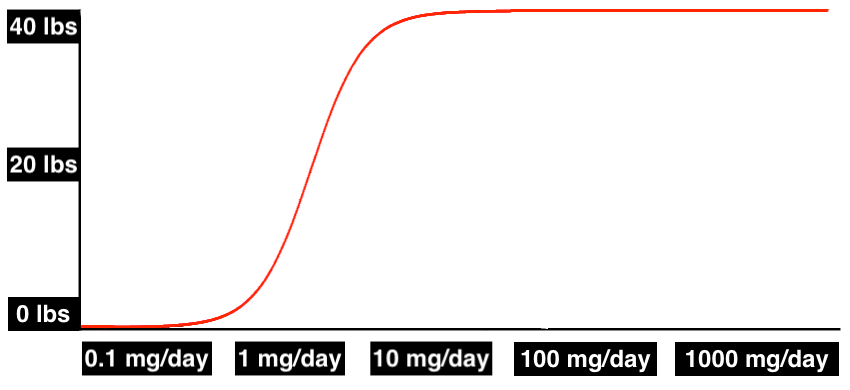
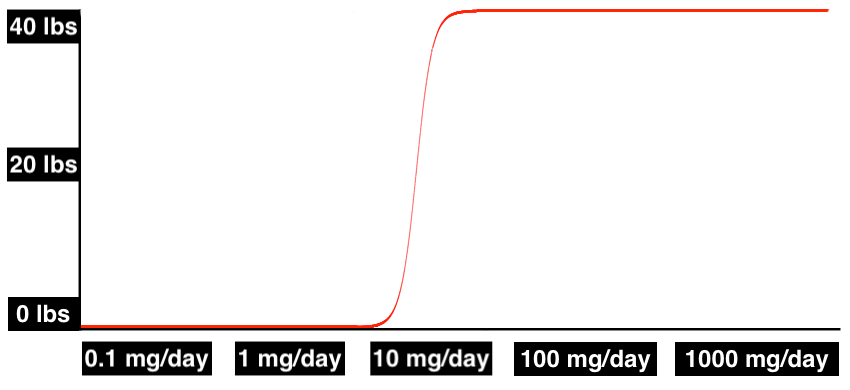
With the addition of these two small steps, she can now use a normal within-subjects experimental approach. Let’s imagine she finds that there’s an 80% chance of developing a migraine on days when she takes no magnesium, and a 30% chance of developing a migraine on days when she takes 400 mg magnesium. She can demonstrate this difference to an arbitrary level of precision, just by running the trial for more days.
Emily’s data might look something like this. The data shown here is not quite enough to reach statistical significance (χ2 gives p = .051) but it’s looking pretty good for 30% chance of migraines with magnesium and 80% chance without.
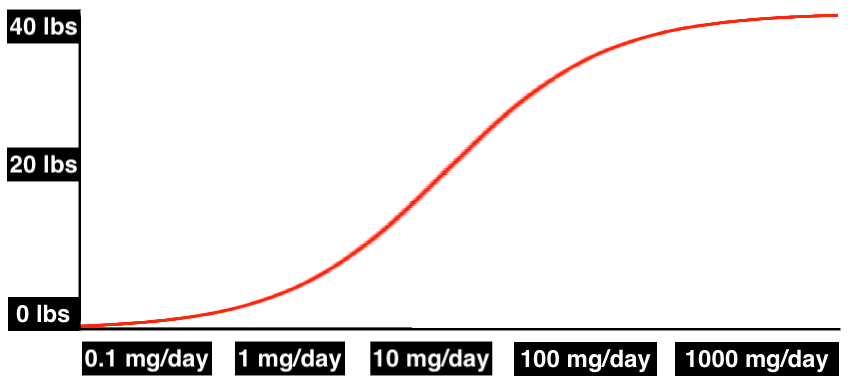
Even if the difference is much more subtle — perhaps a 75% chance of a migraine with 400 mg magnesium and 80% without — with enough days, she can still show to an arbitrary level of confidence that the magnesium has the observed effect FOR HER, however small that effect might be.
This wouldn’t provide any evidence that magnesium will work for anyone ELSE’s migraines. But even if it doesn’t generalize at all to anyone else, Emily can get as much evidence as she wants that it’s really doing something for her. And that still helps the community, because it shows that the treatment works at least sometimes, for some people.
This is different from a traditional case study. Even though it’s looking at just one person, it uses experimental techniques. Compared to a traditional experiment, you sacrifice external validity (will this generalize to anyone other than this one person?) but you still get the same level of statistical rigor and you can still clearly infer causality.
And with this design, you should be able to use standard within-subjects statistical approaches. A sample size of just one is unusual even for a within-subjects study, but not entirely unheard of.
This approach is under-used in the internet research community (though Scott Alexander did one here and Gwern did one with LSD). Lots of people are online sharing tips and tricks on things they think might help their reflux/migraines/IBS/heart palpitations/executive function/etc. This is good, but it’s hard to know which recommendations are solid and which are just random chance.
If you run a within-subject self-experiment, you can do something incredible for your community. It may not help everyone, but you can demonstrate whether it works for you. Publish your null results too — if you suspect that caffeine triggers your reflux, but under close inspection the hypothesis falls apart, report that shit!
We should emphasize that N = 1 studies falsify a very specific kind of null hypothesis: that an intervention cannot work. If the intervention works for you, that just shows that the intervention can work.
It might not work for anyone else, and with N = 1 you have a much higher chance that one person will do something idiosyncratic that makes it look like the intervention was successful, when in fact it was the idiosyncratic thing doing all the work. For example, maybe on days you take magnesium, you always take it with a big glass of lemonade. It turns out the lemonade is what’s helping your symptoms, not the magnesium, and this wouldn’t be apparent from the data, because the lemonade and the magnesium are confounded.
If you want to go above and beyond, you can get a couple friends and do an even more compelling test with only a few people. As long as you all do multiple trials, your effective sample size from a statistical standpoint can still be arbitrarily large. With more people, we have greater certainty that there isn’t something weird confounded with the experimental variable (but never 100%). Every chronic illness subreddit should be generating research pods of 2-10 people, and testing the treatments they think are worth investigating.
Limitations
Even with better randomization, however, these designs still have a lot of limitations.
For a start, they’re limited by the speed of your research cycle. For example, repeated-measures studies won’t work very well for studying obesity, because people tend to lose and gain weight pretty slowly. It may take months to lose and then regain weight, so it’s hard to study weight gain with this method. If you have to randomize periods of months, it will take you a full year to get a sample size of 12. In comparison, headaches would be easier to study, since they come and go daily or even hourly, and you could randomize your treatment on much shorter timescales.
Worse, for some treatments we don’t know what the appropriate timescales will be. Let’s return to Emily and her migraines. If magnesium works on the order of weeks rather than days, she will have to randomly assign weeks rather than days, which means it will take seven times longer to reach an equivalent sample size. But how can she know in advance whether to use periods of days or of weeks?
If a cure is too powerful, or has long-lasting effects, that actually makes it harder to study. If magnesium cures Emily’s migraines for a month, she’ll have to wait a month between randomization cycles, and it will take her years to get a decent sample size.
Similarly, this kind of protocol may not be able to detect more complicated relationships. If Emily’s body builds up a reservoir of extra magnesium over time, this may be difficult to model and might throw off the clarity of the experiment. Or if her body gets more aggressive about clearing the excess magnesium from her system, the magnesium will have less effect over time, and will have even less effect on trial runs where she has multiple magnesium blocks one after another. These designs have a lot to offer, but they’re not going to get us very far in the face of genuinely complex problems.
Another downside of this approach is that Emily has already found a treatment she likes. Probably she would like to take magnesium every day and get as few migraines as possible, but to do this within-subjects self-experiment, she has to try going off the magnesium multiple times over the course of several months, to make sure it really works. We think it’s often worth it to know for sure, but it isn’t easy to stop a treatment that seems to be working.
Finally, the big limitation is that you can only use this approach if you’ve already identified a treatment that you suspect might work for you. If you’re sick and you don’t have any leads, this method can’t help you figure out what to try. It’s only good for testing or confirming hypotheses — it can’t give you any new ones, can’t narrow down a list of cures or triggers out of the huge number of things that might possibly be making you sick.
That’s not much weight loss, but it’s also not a very big supplemental dose of potassium, and the weight loss is significantly different from zero. People who took higher doses of potassium lost more weight, as did people who weighed more to begin with.
But what about past that first span of 29 days? Some people kept going with the protocol, taking potassium up to 60 days. Today we report their data.
30+ Days Results
We took a snapshot of all participants’ data on January 5, 2023. This was more than a month after we collected the data from the first 29 days, so everyone had the opportunity to reach 60 days by this point if they wanted to. This new snapshot is available on the OSF.
All the sample sizes in this case are too small to be statistically significant with the potential effect sizes involved, so we don’t report any statistical tests in this post.
We cleaned these raw data and are going to look at the data from Day 1 on the protocol to Day 60. Some people may have kept going past Day 60, but we aren’t going to look at that right now.
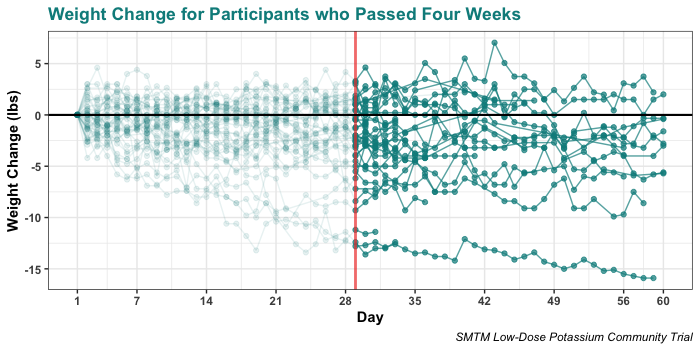
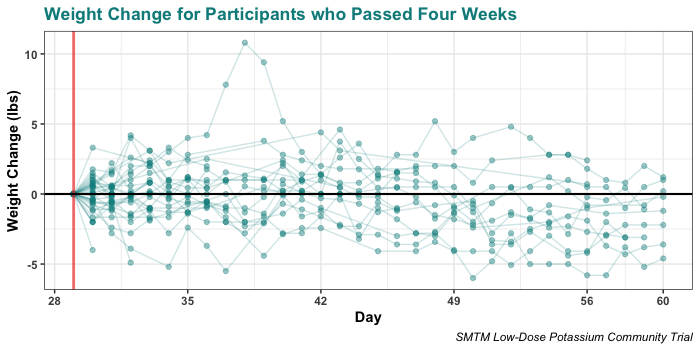
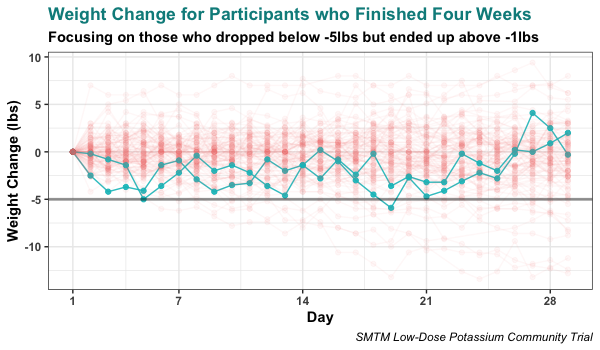
Here are the overall trajectories for the people who reported at least one day’s weight beyond day 29. The vertical red line indicates day 29, so all data points beyond that are past the span of the original trial.
Overall the trend seems to continue. One person ended up down more than 15 lbs, but that’s not at all representative.
People lost weight on average, but we already knew that. In this case we are most interested in whether they kept losing weight past the official end of the trial, so here are those same data zeroed from their weight on Day 29:
We see that in this span, people also lost weight on average, though the average weight loss was not very large. The average weight change past day 29 is negative, -0.37 lbs with all data.
See that spike up to more than 10 lbs? As you may have guessed, those are the days immediately following Thanksgiving. The participant reported that this was their “heaviest weight in 9 years”, but as you can see they lost all that excess weight very quickly.
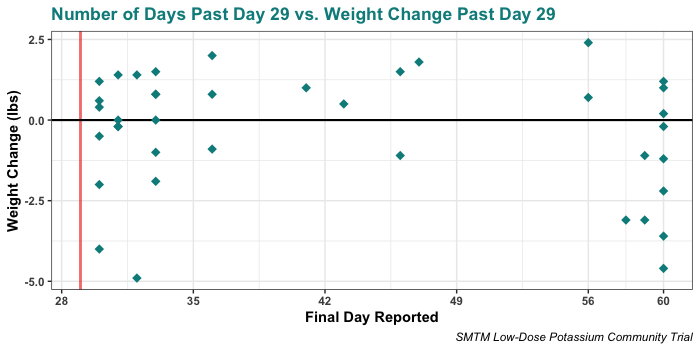
These plots can make it hard to see what has happened for each individual, so let’s now break things down and just show their last reported weights, again relative to their weight on Day 29.
Here’s a plot of each person’s last reported day, and their reported weight change as of that day.
You can see that there are roughly two groups — most people either made it just a few days past Day 29, or made it up to very close to day 60.
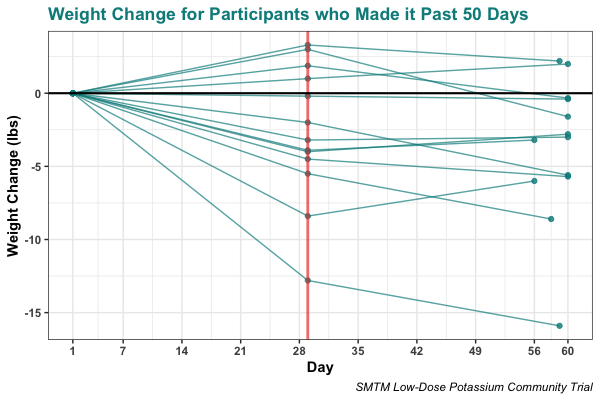
We can take a special look at that second group, people who made it to Day 60 or nearly did so. Here’s everyone who made it past 50 days, broken out by just the landmark measurements — their weight on Day 1, on Day 29 at the official end of the trial, and on the last day they reported.
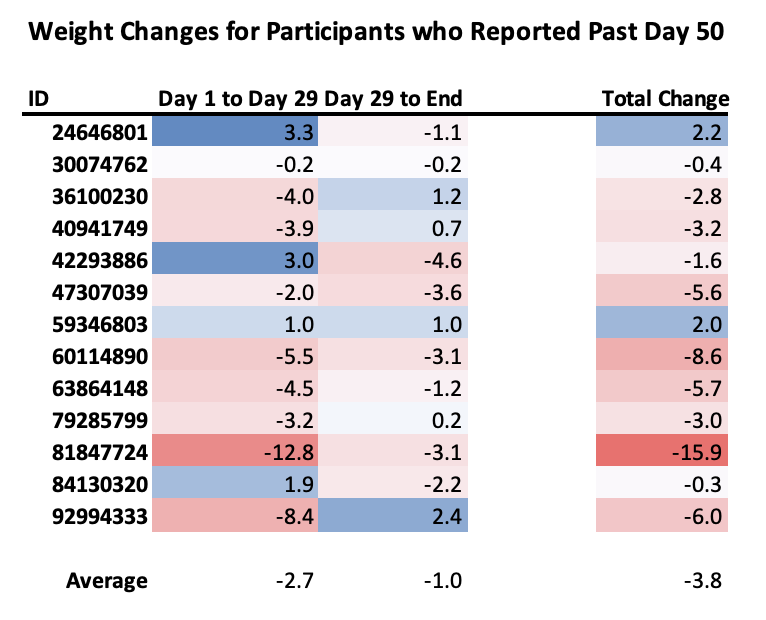
And here are those same data as a table:
On average, these people lost a decent bit (2.7 lbs) in the first span of the trial, and less in the second span (1.0 lbs). But this obscures a lot of individual stories that are more extreme in one way or another, like participant 42293886, who gained 3 lbs in the first leg but lost 4.6 lbs going to day 60, for a total change of 1.6 lbs. (This participant told us, “Not going to go off potassium any time soon I suspect. Making a little effort to lose weight, and it’s showing a small amount of success.”)
Also notable is that the only two people who had net weight gain by 50+ days are people who had already gained weight by day 29.
Summary
Probably the people who kept going past Day 29 were the ones who were most motivated, or who had seen the best results up to that point, so there may be some selection bias.
While none of this is super compelling, people who kept going did on average keep losing weight. They didn’t stick right where they were on Day 29 and they didn’t regress back to the mean. It’s a small amount more evidence in favor of the idea that supplemental potassium might cause weight loss, another tiny pebble on the scale.
In a practical sense, we still recommend that anyone who wants to lose weight should go on the potato or half-tato diet. It’s much more reliable, and more delicious.
Research methods are still very new, probably we can sit down and invent some more.
This is good news, because right now there are many problems that we have no idea how to solve. One area of particular mystery is human health. Doctors can do a lot for you with surgery, vaccines, and antibiotics, but outside of these interventions there remain many ailments that totally stump the system.
A weird part of the postmodern experience is that many people feel kinda bad all the time, even if they aren’t “sick”. If you go to the doctor and you’re like “I’m feeling kinda bad”, they don’t know how to help you.
Being “actually sick” doesn’t get you much further. If anything it’s worse. Lots of people have mystery chronic illnesses, but when you go to doctors with one of these problems, they mostly just shrug at you.
II.
Alistair Kitchen began having stomach pain. It started out small, but over time grew to “an intensity of pain I didn’t know my body was capable of producing, a literally blinding sensation that shut down every sense in my body except the sensations of my stomach.” He says:
So, four years of this. In the third year, after an endoscopy and a series of scans had cleared me for anything “serious”, the advice given to me was, essentially, this:
Look, some people just have trouble with their stomachs. When they have trouble and we don’t know what is causing it, we just call it IBS. So you have IBS. Watch out for foods that might trigger you, and good luck.
Me (over 20 pages of medical history and 30 minutes of conversation): I can’t digest protein or fiber, when I try it feels like something died inside me.
Them: Oh that’s no good, you need to eat so much protein and vitamins
Me: Yes! Exactly! That’s why I made an appointment with you, an expensive doctor I had to drive very far to get to. I’m so excited you see the problem and for the solution you’re definitely about to propose.
Them: What if you took a slab of protein and chewed it and swallowed it. But like a lot of that.
Me: Then I’d feel like something died inside me, and would still fail to absorb the nutrients which is the actual thing we want me to get from food.
Them: I can’t help you if you’re not willing to help yourself.
Having faced this system, many people end up taking their health into their own hands. This makes a lot of sense and we fully endorse it. But most people have no more success on their own than they do with doctors (though at least they’re not being condescended to).
It seems like the average outcome is that you end up living with your mystery illness (or even just your mystery sense-of-mild-feeling-bad-all-the-time) for years. It either never goes away, or randomly goes away some day for no apparent reason.
III.
We suspect that people do about as well on their own as they do with doctors because *no one* knows how to study individual issues. This is because our civilization has done a good job developing population-level research techniques, but a crummy job so far coming up with individual-level research techniques.
Our society has devoted a lot of time to doing research on large groups. We’ve come up with lots of ways of running studies on large samples, and lots of ways of thinking about it. We’d bet that 99% of the studies you’ve ever read are studies on groups.
In comparison, doing research on individuals is a very understudied and (dare we say) cutting-edge form of research. Scientists mostly haven’t developed techniques for it, because almost by definition, it isn’t the kind of thing they study.
Possibly this is because doctors and researchers are more interested in population-level issues. After all, they are usually tasked with solving public health crises, tasked with curing common diseases, things that might affect millions of people. But individuals care more about, well, individuals.
Possibly this is because we started by focusing on the most common illnesses and are only now getting around to the rare ones. Common illnesses are best studied by looking at large groups, so we developed those techniques first, and are only now running up against their limitations.
Possibly it is all a question of computational power. The history of statistics is tainted, because statistics was invented before computers, and was designed within the limits of what a person can reasonably calculate by hand. Even up to the 1990s, consumer machines would take weeks to crunch the kinds of models that today you can run in 15 minutes on your phone. But now we can do more, and maybe that means we can do new things, things that weren’t possible before.
In any case, it must be possible to come up with protocols for such a thing.
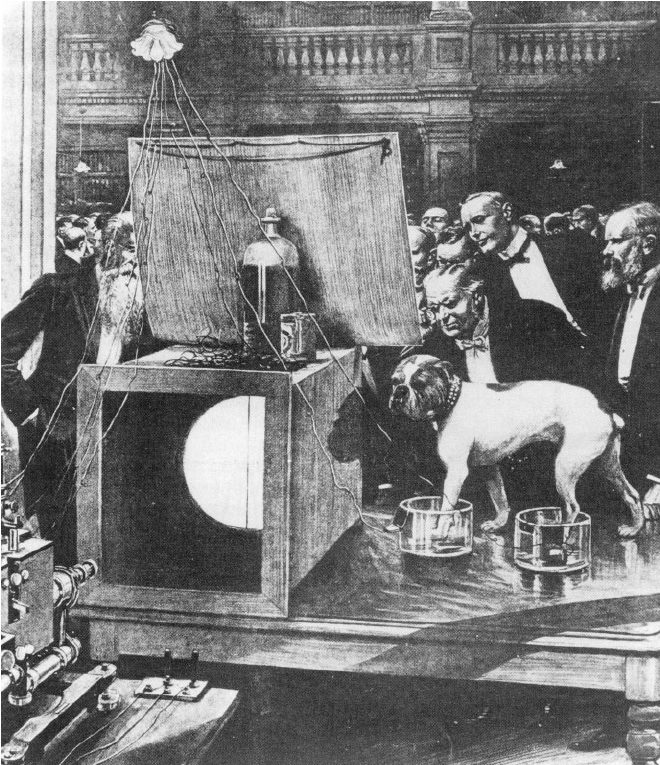
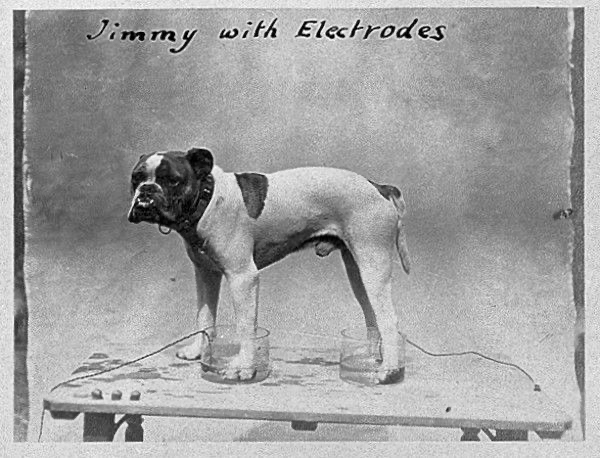
“Jimmy with Electrodes”
Individual-level research comes with certain advantages. The problem with population-level techniques is that the same treatment will always work better for some people than for others. If you give two people the same drug, it might work great for one of them and not work at all for the other, and your statistical modeling needs to take that into account. Individual-level research doesn’t have to worry about that! You are just looking at one person.
A technical way of describing this is that individual-level research always has high internal validity — the research question is “does this treatment protocol work for this person” and you always get a straight answer to that question. This comes at the cost of external validity — you have basically no idea whether your findings will generalize to any other person. That’s an ok tradeoff, because you are already choosing to study an individual, and because population-level techniques have questionable external validity to begin with.
We may also be able to use population-level techniques to guide individual-level research, and individual-level techniques to guide population-level research; there may be many ways in which they are complementary.
Individual-level techniques won’t be limited to studying chronic illness — you could also use them, for example, to make healthy people feel amazing more often, which would be pretty cool. People who already feel amazing all the time, you’re on your own.
But chronic illness is a good place to start, because these illnesses are a drain on the lives of millions of people who are motivated to figure out a treatment, and population-level medicine isn’t cutting it.
This is a problem we have been mulling over and that we will be writing about over the next couple months. To start with, here are some simple distinctions that seem like they might come in handy:
Testing vs. Finding Variables
When studying an individual, there are two main situations.
One situation is where you think you know some variables that are involved with your illness, and you want to test them. For example, you may suspect that caffeine makes you feel nauseous. You want to confirm this hypothesis or rule it out. You might also want to demonstrate to a high degree of certainty that caffeine is really a trigger for you, so you can write about it on the internet and other people with random nausea can benefit from your example, possibly by trying it for themselves.
The other situation is where you have no idea what is causing your illness. When you have no clear leads, you want techniques that can help you find variables that might plausibly be involved. This is a much harder problem, but it’s also much more important, because many people are chronically sick and have no idea what is causing their illness.
This sucks, and it’s very tricky because there are approximately infinity variables in the world. But probably we can do better than “try variables at random” (even if some level of luck is inevitably involved), and we should see if we can come up with techniques for this situation.
Triggers vs. Deficiencies
Sometimes a chronic illness is caused by getting too much of something, like an allergen. These are generally known as triggers. Sometimes a chronic illness is caused by not getting enough of something, like a vitamin. We call these deficiencies.
This distinction seems like it might be helpful, because the techniques for finding triggers may be very different from the techniques for finding deficiencies. (More on this in future posts.)
We should also keep in mind that chronic illnesses can be more complicated than simply getting too much or too little of something. Some chronic illnesses aren’t caused by any external variable — there’s always the possibility that you have a brain tumor or something, in which case there may be no triggers or deficiencies involved.
Ruling In vs. Ruling Out
Sometimes we will be in the fortunate position where we can get a lot of evidence that X causes Y. If we can conclusively pin things down and show that dairy causes your chronic nausea, that’s great. Now you can keep yourself from feeling sick all the time, and that’s enormously valuable.
But sometimes we won’t be able to get evidence in favor of anything — we will only be able to disprove things. It’s important to remember that this is valuable too. Maybe you suspect that your nausea might be caused by dairy, caffeine, alcohol, or fatty foods. If you go through them one by one and rule them all out — nope it’s not dairy, it’s not caffeine, not alcohol, not fatty foods — that’s still good to know.
It will be disappointing that you continue to feel nauseous all the time and you don’t know why. It may feel like a step backwards, because you’ve ruled out all your best guesses. But it’s still enormous progress. Disproving a hypothesis is valuable, and at least now you’ll be able to enjoy your milkshakes, Irish coffees, and beer-battered onion rings without fear.
The best thing research can offer you is a cure, but the second-best thing it can offer is some peace of mind.
Companions the creator seeks, not corpses, not herds and believers. Fellow creators the creator seeks—those who grave new values on new tablets. Companions the creator seeks, and fellow harvesters; for everything about him is ripe for the harvest.
— Friedrich Nietzsche, “Thus Spoke Zarathustra”
There’s a long tradition in the history of medicine where people figured out the cause of an industrial disease by noticing that one profession had a much higher rate of the disease than everyone else. For example, in Victorian and Edwardian England, chimney sweeps had a rate of scrotal cancer more than 200 times higher than workers who weren’t exposed to tar on the job. No, we are not making this up.
Now it’s your turn to do something similar. Your mission, should you choose to accept it, is to write a review of the mysteries on a topic and send it to us at slimemoldtimemold[at]gmail[dot]com by July 1st 2023.
Pick a topic, and write about the mysterious aspects of that topic, like we did for the mysteries of obesity in Part I of A Chemical Hunger. We mostly expect you to review topics from “hard science” areas like medicine, biology, chemistry, and neuroscience, but we are open to reviews of mysteries from social science, economics, political science, or the humanities. If you feel you can make a strong case for some mysteries and why they are mysterious, that’s good by us.
You can include Normal Mysteries, things that are unexplained but that most people know about and don’t seem all that confusing. For example, IBS and migraines are about 2-3x more common in women than in men. Everyone kind of knows this, so it’s not all that weird, but no one can really explain it, so it is still a mystery. The first three mysteries we reviewed about the obesity epidemic were all pretty normal.
You should also review Weird Mysteries, things that most people aren’t aware of and/or that seem like they totally don’t make sense, things that fly in the face of our understanding. The rest of the mysteries we reviewed about the obesity epidemic were pretty weird, like how lab animals and wild animals are also getting more obese. What’s up with that?
Our hot tip is that the simplest form of mystery is just unexplained or unexpected variation. A good example is how obesity rates vary by altitude — low-altitude counties in the United States have much higher obesity rates than high-altitude countries do. This is not predicted by most theories of obesity, and many people found this very surprising.
An unexpected LACK of variation can also be a mystery. For obesity, it feels intuitive that people who eat different kinds of diets should weigh different amounts, but diet consistently seems to make very little difference. From the perspective of the mainstream understanding of obesity, this is pretty mysterious.
How do you know that you’ve found a good mystery? It’s an emotion, a feeling that starts in your gut, not unlike IBS (which, hey now that we think about it, is pretty mysterious). Start with something that you just can’t wrap your stomach around. We’re looking for a confusion that started rumbling in your tummy when you were a student who kept asking the same basic questions and couldn’t get a straight answer, a confusion that has just kept grumbling away right there next to your esophagus ever since — now that’s a mystery. The best mysteries will be assumptions where everyone else thinks everything is fine, but you have a nagging suspicion that something is wrong.
Please focus on the mysteries of your chosen subject — DO NOT include a theory. If you feel you need to provide context, you can discuss popular theories and how your mysteries support or undermine them (like we did in Part II). But no arguing for a theory or introducing a theory of your own.
This is a mystery contest, not a theory contest. Your mystery review is the hook; if you do a great job reviewing some mysteries and win the contest, everyone will be excited to hear about your theory. Then you can put it on your own blog and get a lot of readers. If people think you have a promising direction, maybe you can get funding to study it further.
Software engineers who have just lost their jobs; grad students on strike; academics who are fed up with the paywall curtain; couples who have just retired at 35; founders whose last venture was recently acquired; billionaire playboys with too much time on their hands; anyone who is looking to make a pivot to research — this is the contest for you. You don’t need a lot of research chops to look at something and tell that it’s weird; anyone can pick out mysteries by noticing when things don’t add up, when things are unexplained, or when experts all disagree on the best explanation.
If anything, outsiders and newbies have an advantage. If your career doesn’t rely on pretending to understand, it’s easier to spot things that don’t make any sense.
Don’t do this though
Contest Format
We have recruited some judges to help us evaluate the mysteries: Adam Mastroianni, Lars Doucet, Applied Divinity Studies, Tony Kulesa, and possibly some other judges TBA. We will consult with these judges and will choose around 5-10 finalists, which will be published on the blog. Then readers will vote for the best. First place will get at least $2000, second place $1000, third place $500, though we might increase those numbers later on.
Use your expertise. The best entries will probably be about things YOU are already familiar with, things where you know about the mysteries the rest of us haven’t noticed yet.
All forms of media are welcome! We like to write really long stuff, and sometimes we just post our correspondence. But if you like to boil ‘em instead of mash ‘em (or stick them in a stew!), that’s cool too. Podcasts, videos, slideshows, semaphore code, etc. are all welcome. All written finalists will be published on the blog. Finalists in other formats (e.g. videos, podcasts) will be linked to. The language shared by the judges is English, so we prefer materials that suit the conventions of English speakers.
You must submit your entry under a pseudonym. This helps people discuss you and your work without having to say, “the guy or lady perhaps or person or team who wrote the SMTM mystery contest entry on pancreatic cancer”. Instead they can say, “blorpShark’s wonderful mysteries of pancreatic cancer review”, which is much nicer.
Pseudonyms also keep famous people from having an advantage. For this reason, if you already go by a well-known pseudonym on the internet, please choose a new pseudonym for this contest.
Team submissions are strongly encouraged (friendship is the most powerful force in the universe), and we encourage you to pick a band name. Go to your nearest band name generator and pick the stupidest name it generates. For solo entries, we recommend a rap name generator, like Post Malone did.
After the contest is over, if you want to connect your pseudonym to your other name(s), please feel free to do so. If you do not provide a pseudonym, one will be provided for you.
If you submit a non-written entry, please send it to us in a form that is as anonymous as possible. For example, you might send a podcast entry as an audio file, or a video essay as a video file. Don’t mention your name in the recording, etc.
Please submit written entries by putting them in a Google doc and sharing that doc with us. We will try to preserve your formatting as best we can if we publish your entry as a finalist, but no promises. If you want to make sure your formatting appears as intended, use simple formatting (e.g. bold, italics, and images). The more complicated your formatting is, the more likely we are to make an error in copying it over.
Please don’t put your name or any hints about your identity in the Google doc itself. If you do, we may remove that information or disqualify your entry.
Please make sure that the Google doc is unlocked and that we can read it and share it with the other judges. Go to the “Share” button in the upper right, and on the bottom of the popup click on where it says “restricted” and change to “anyone with the link”. If you send us a document we can’t read, we will probably disqualify you.
Frankly we reserve the right to disqualify entries for any reason, or no reason at all.
If you win, we will send you your prize money in the form of an envelope stuffed with cash, or something else if we agree that it’s more convenient.
Your due date is July 1st, 2023. If you have any questions, ask in the comments so other people who have the same questions can see. You can also email us or ask us questions on twitter. Good luck!
We commented on this in an earlier links post, now Aella goes off on the same point: You don’t need a perfectly random sample for useful data, jfc. She’s right by the way, as is Scott Alexander. See also Eigenrobot on twitter: “the biggest problem in both statistical practice and criticism of statistical practice is braindead insistence on following form rather than consideration of whether adherence to form is sufficient to produce the desired insight or necessary to produce any insight respectively”
@selentelechia on twitter has been trying an “old 4chan iodine theory on fast food salt cravings”, which is about as crazy as it sounds, but she’s experienced some pretty good outcomes: “I’ve been doing this for two days and my hands aren’t cold anymore, nor are they taking half an hour to warm up after coming inside … I don’t feel a constant low level impulse to lie down”. Seems interesting.
“Many cell lines that are widely used for biomedical research have been overgrown by other, more aggressive cells,” begins Wikipedia’s list of contaminated cell lines. “For example, supposed thyroid lines were actually melanoma cells, supposed prostate tissue was actually bladder cancer, and supposed normal uterine cultures were actually breast cancer … Estimates based on screening of leukemia-lymphoma cell lines suggest that about 15% of these cell lines are not representative of what they are usually assumed to be. … Contaminated cell lines have been extensively used in research without knowledge of their true character. For example, most if not all research on the endothelium ECV-304 or the megakaryocyte DAMI cell lines has in reality been conducted on bladder carcinoma and erythroleukemia cells, respectively.” (h/t @MasterTimBlais)
@goblinodds asks twitter, “do both of your eyes see the same colors or is one’s input cooler-toned than the other?”, finds that 20.9% report different temperature input from different eyes. Uh???
“Many researchers have conjectured that the humankind is simulated along with the rest of the physical universe – a Simulation Hypothesis. In this paper, we do not evaluate evidence for or against such claim, but instead ask a computer science question, namely: Can we hack the simulation?” Science Banana draws particular attention to Table 1:
Great bloggers are rare, weird, and not team players. Showing our biases here, but we actually think that this is an argument for teams of bloggers, like yours trulies. For one person to be a great blogger they may indeed need to be obsessed about writing all the time & very widely read & interested in just about everything & willing to work for relatively low wages, but if your blogging team is two people, you only need to have that combination of traits between the two of you. If you can make a blogging collective of four people, you only need one person who has each of those traits! Maybe it’s a crazy scheme but we’re the ones with the hive mind over here.
In November 2021, we finished our series A Chemical Hunger, where we argue that the obesity epidemic is the result of environmental contaminants, and that one of those contaminants might be lithium. We hadn’t really expected anyone to read it. But we were wrong — tens of thousands of people have now read the series, and to date the twitter thread giving an overview of the series has more than 2 million views.
In April 2022, we announced the Potato Diet Community Trial. We expected that the potato diet would be really hard to stick to and people would only lose a little weight, if any. But we were wrong — people said the potato diet was easy, enjoyable, and on average, people lost 10.6 lbs over 4 weeks.
Potatoes are really high in potassium, so we wondered if potassium could be the active ingredient causing the weight loss in the potato diet. We decided to try a self-experiment where we took small amounts of potassium salt every day, but it seemed unlikely that such tiny doses could have any effect. But we were wrong — we each lost about 5 pounds over four weeks. One of us kept going and lost 12 lbs over 60 days.
The goal of this study is to see if the large doses of potassium found in potatoes could plausibly be the reason why people lose weight on the potato diet.
The doses of potassium in this study are small in comparison to the potato diet, only a few thousand milligrams per day. This is much less potassium than people got on the potato diet, so we don’t expect the effect to be large in any practical sense. In fact, we expect that if there is an effect at these doses, it will be quite small, probably a loss of only a few pounds on average. We are just looking to try to see if there is any effect at all.
Potato diet estimate per the USDA’s estimate for potassium in 2000 calories of potatoes
We are studying potassium because it is a major variable from the potato diet that we can easily look at in isolation, not because we think potassium will be a great or a practical treatment for obesity on its own.
We don’t expect everyone to lose weight on this protocol, or for it to be sustainable in the long term. We just want to know if potassium could be the reason why people lose weight on the potato diet, something that we currently have almost no information about. If it looks plausible, that tells us something about why the potato diet works; and then we can consider, ok wait a minute, why would potassium cause weight loss at all? But more speculation on these points after we look at the results.
Raw data, the analysis script, and study materials are available on the OSF. The dataset is very rich and there’s a good chance that we haven’t found everything there is to find. So if you are statistically inclined, after you’ve finished reading this post we encourage you to download the data and have a look for yourself. If you find anything interesting, or even if you’re just able to confirm our findings, you should write up your analysis on your own blog and let us know about it! Science is a game, please play!
If you recreate these analyses at home, your results may be slightly different than ours because three participants asked that their data not be shared publicly.
Whether or not you like what we’ve done here, we encourage you not to take our word for it. Download the data and materials, perform your own analysis, share your criticisms, run your own study. If you think you can do a better job, maybe you are right! Show us how it’s done.
2. Variables
We collected variables at three points.
First, we collected demographic variables at signup. The variables we collected at this point were:
chromosomal sex
reported hormone profile (so we can distinguish trans participants with less ambiguity)
age in years
profession
race/ethnicity (from a limited number of options)
local postal code
current country of residence
whether they had done any sort of potato diet in the last year
In response to this last question, the majority told us they had not done any potato diet in the last year, but 40 told us they had done some kind of potato diet on their own, and 7 said they took part in our Potato Diet Community Trial.
After signup, we had people track a number of variables about their health and their diet (and how much potassium they were taking) over the course of the study, on a spreadsheet we provided. You can view a version of that spreadsheet here.
The main variables collected on this sheet were:
weight (in the morning)
potassium doses (up to four doses a day)
variables for whether or not participants consumed meat, eggs, dairy, leafy greens, and tomato products each day (just a 1 for “ate it today” and a 0 for “didn’t eat it today”), because we suspect these foods may be high in lithium (though we’re not sure)
We also included fields for several bonus variables, which were optional but encouraged. These variables were:
calorie intake
waist circumference (which a couple people asked for after the potato diet)
sodium intake
energy, mood, and ease of study (all on 7-point scales)
systolic and diastolic blood pressure
total Cholesterol, as well as LDL and HDL cholesterol
triglycerides
resting heart rate
fasting blood glucose
body temperature
estimated hours of sleep the night prior
sleep quality the night prior
fidgeting (on a 1-7 scale)
estimated minutes of exercise
(and several fields for notes)
After we took a look at the data, we realized we had a few questions about aspects of the study that we hadn’t really measured. For example, some people mentioned that they hated the potassium while other people mentioned finding it delicious. But most people didn’t mention this aspect at all, so it would be hard to conduct any analysis related to how much people enjoyed the potassium.
So finally, on December 3rd, we sent a followup survey asking about some of these remaining questions. Five days later, there were 105 responses. We downloaded these responses and added them to the dataset.
The variables we collected at this point were:
what potassium compound they had primarily consumed
what form they had taken it in (e.g. salt vs. capsule vs. tablet)
what brand of potassium they had primarily consumed
what delivery methods they had used (e.g. in food vs. in a drink)
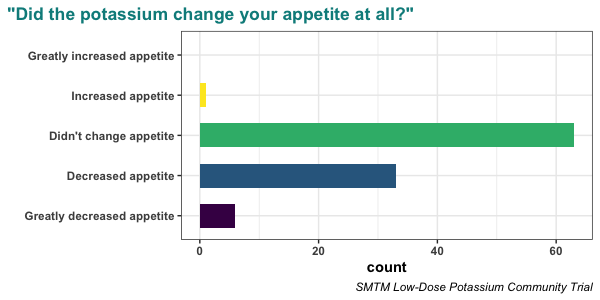
change in their appetite
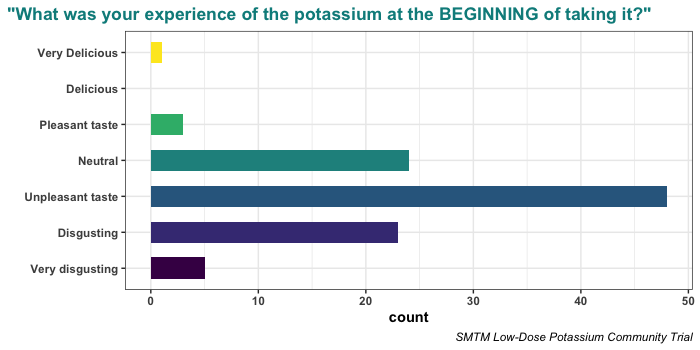
how much they enjoyed the potassium at the beginning of the trial
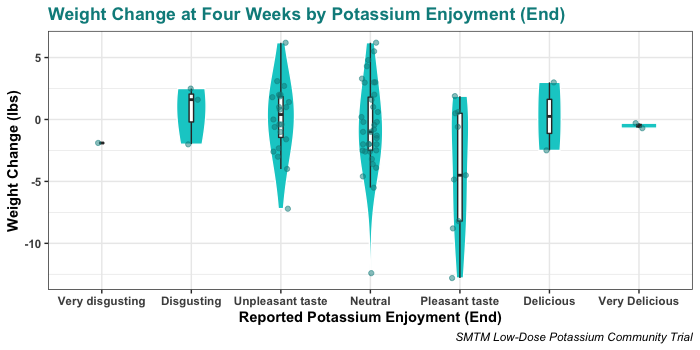
how much they enjoyed the potassium at the end of the trial
whether they felt leaner or chubbier subjectively
whether they were intentionally exercising or eating more or less during the trial
whether they were on some other diet or routine when they started the potassium trial
and a free-response question asking if there was anything else we should know
For more detail, see the copies of the materials available on the OSF.
3. Protocol
As a reminder, the main study protocol was:
Start with two doses of 330 mg potassium (1/8 tsp Nu-Salt) on the first day.
If you feel fine, try three or four doses of 330 mg potassium (1/8 tsp Nu-Salt) on subsequent days.
If you’re feeling fine after 4-7 days, try one dose of 660 mg potassium (1/4 tsp Nu-Salt).
If you still feel good, keep increasing your dose by small increments. For example, if you are on two doses of 660 mg (1/4 tsp Nu-Salt) a day, you might increase that to three doses of 660 mg, or one dose of 660 mg and one dose of 1300 mg (1/2 tsp Nu-Salt). If a higher dose makes you feel bad, try returning to the dose you were on before and maintain that.
Try slowly increasing to two doses of 1300 mg (1/2 tsp Nu-Salt) a day. Only go beyond that if you are feeling totally fine.
You should calibrate based on your own experience — different people will have different needs and different limits. For example, we’d expect someone who weighs 300 pounds would be able to tolerate higher doses than someone who weighs 150 pounds.
If you feel weird / bad / tired / brainfog and you can’t tell why, try:
eating something;
drinking some water;
getting some sodium;
and see if any of those help. It may be easy to end up needing food / water / salt and not notice.
If you still feel weird, try dropping to a lower dose or taking 1-2 days off.
If at any point you feel sick or have symptoms of hyperkalemia, stop immediately and seek medical attention.
Participants were asked to record their weight every morning, and they were asked to record data up to the weight measurement on the morning of day 29 regardless of whether they stuck to the protocol. That way even if someone found the potassium intolerable, we could still use their data.
4. Participants
A total of 305 people submitted the initial form.
Of those, 15 people filled out the signup form incorrectly in such a way that we couldn’t sign them up (they didn’t enter an email, didn’t enter critical data such as height, etc.). We enrolled the remaining 290 people in the study.
Of the 290 people who were enrolled, 57 never entered any data on their spreadsheet, leaving 233 people who entered at least one day of weight data.
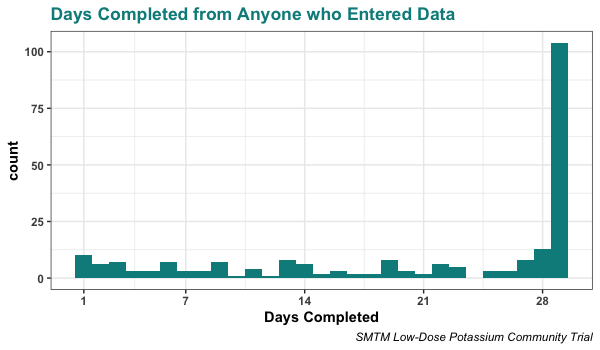
The most common outcome in this group was to make it the full 29 days, but the majority of the 233 people who entered data on day 1 stopped entering weight data before day 29. Here’s the distribution of days completed (as measured by last weight entry) from that group:
As shown above, 104 people entered weights on both the first day and on day 29. This was the criteria we specified in advance for the group we would focus on for the main analysis. Specifically, we said:
Anyone who records data for 29 days is clearly taking the study seriously, even if they weren’t able to stick to the potassium supplements the whole time. … Based on this, our main analysis will focus on participants who provide 4 weeks of data. If you provide a weight measurement for the morning of day 1 and the morning of day 29, so we can calculate your weight before and after, and you took at least one dose of potassium, we will do our best to include you in the analysis.
5. Weight Loss
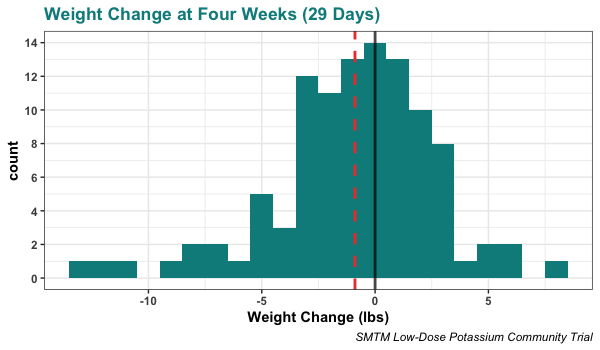
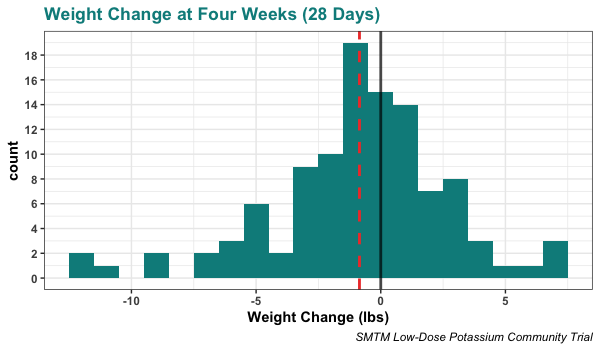
The main outcome of interest is weight change by the morning of day 29. Here’s the histogram of that variable, with a black vertical line at 0 lbs (i.e. no weight change over 29 days) and a red dashed vertical line at the mean weight change:
On average, people lost weight. The mean is -0.89 lbs, or an average loss of 0.89 pounds over 29 days. With a sample size of 104, this is significantly different from zero in a one-sample t-test, p = .014, and the 95% confidence interval for average weight change is [-1.59, -0.19] pounds.
However, this obscures the data of several people who made it to the end of the study, but who mistakenly didn’t report a measurement on day 29. If we look at the data of everyone who reported a weight on day 28, this is the histogram:
This has a mean of -0.85 lbs and a larger sample size, and is also significant, p = .016.
The same thing is true if we look at everyone’s weight at day 27 — the average weight loss is 0.86 lbs and this is significant, p = .016. The exact cutoff doesn’t matter, which indicates that the result is robust.
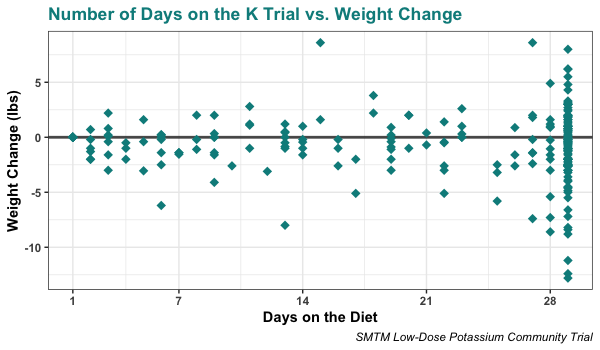
People who dropped out before reaching the end of the four weeks also seem to have lost weight on average. You can see that the majority of people who stopped before day 21 are below zero (the horizontal line), indicating they lost some weight over the time they spent on the trial:
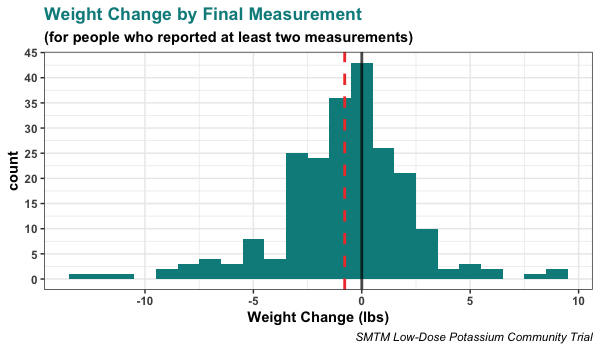
In fact, if you look at the weight change from EVERYONE who reported at least two weight measurements (i.e. not including those people who only reported weight for day 1, who literally could not have seen weight change), people still lost 0.79 lbs on average. Here’s the histogram:
Because of the much larger sample size, this is still significant. In fact the p-value is quite a bit lower (p = .0002) and the 95% CI is noticeably narrower, [-1.20, -0.38] pounds.
The average weight loss here is smaller, but remember that about half of these people did not make it the full four weeks! In fact, this analysis includes 26 people who didn’t even make it 7 days.
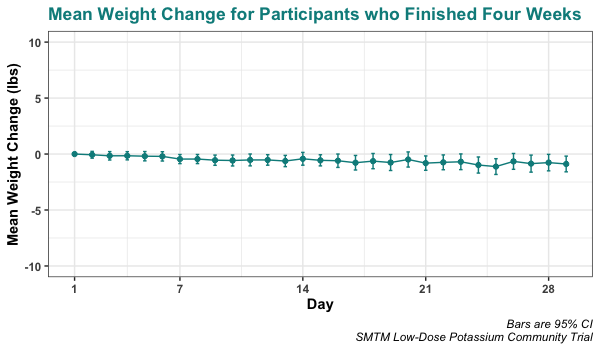
Looking over the course of the study as a whole, it appears that people slowly lose weight over time, with no apparent changes in the trend:
Of interest here is that the 95% CI excludes zero for the first time on day 7, and that day 25 is the point of greatest average weight change.
Looking at individual trajectories is a right mess, but here’s the plot anyways:
Causes
On average it looks like people lose about 0.8 lbs over four weeks on this protocol. This isn’t much weight loss, but it’s statistically distinguishable from nothing.
But obviously some people do lose more weight, sometimes a lot more. Three people lost more than 10 lbs. It’s clear that there is a lot of variation around the small average weight loss. Can we figure out what caused any of this variation?
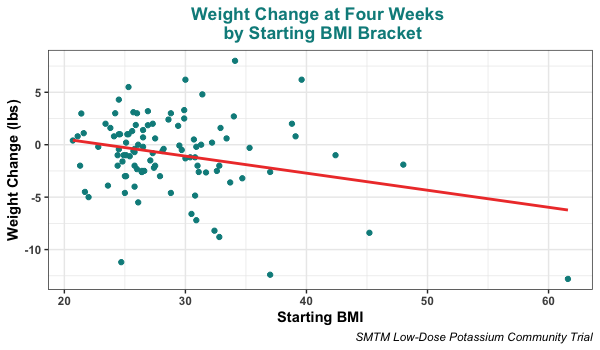
Well for one thing, some people did not have much weight to lose to begin with. Here’s weight change on day 29 compared to starting BMI:
As you can see, people who started with higher BMIs lost more weight. This correlation is significant, r = -0.269, p = .006, and is exactly what we would expect. People who have a BMI of 22 don’t have much weight to lose, so we should expect to see very little weight loss from them, perhaps no weight loss at all. Meanwhile people with higher starting BMIs have more to lose. It’s interesting to see that the person with the highest starting BMI also lost the most weight.
Many lean people participated in this study, and most seem to have signed up because they wanted to contribute to the research even if they were unlikely to lose weight. This isn’t an experiment, but some of them do provide a sort of baseline response. “I am happy with both weights,” said one participant, “and wasn’t expecting or hoping for a big weight loss number. I thought of myself as somewhat of a ‘control group.’”
If this were a “normal” study, and we were “normal” researchers, we probably would have restricted signups so that only people with a starting BMI of 30 or higher (technically obese) could sign up for the study.
If we had done that, here’s what the analysis would look like. Unsurprisingly, this group lost more weight on average:
The average weight loss for participants who started the trial with a BMI of 30 or above was 1.83 lbs, and again this is significant, p = .031.
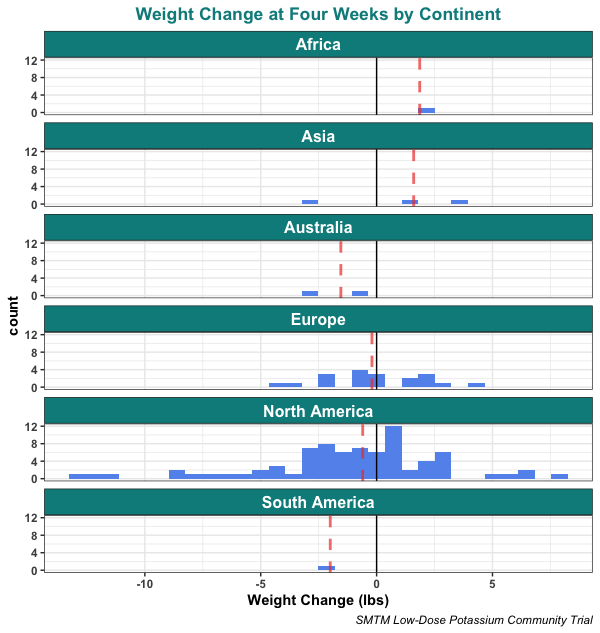
Another thing that might matter is what country people are from. This is especially interesting from the perspective of the contamination hypothesis, because we suspect some countries have more contaminants than others. We tried doing a “USA vs. all other countries” analysis, but that was not significant, p = .341. There also doesn’t seem to be a clear effect of what continent people are on, but we can still plot these data:
Nothing groundbreaking here, but we do want to note that we see much less variation in Europe than in North America.
But of course, the main thing we should expect to make a difference in the results of the potassium trial is the amount of potassium!
In this study, everyone was on the same protocol, but some people took much more potassium than others. People were asked to start with two doses of 330 mg on the first day and slowly work up to two doses of 1300 mg a day, but they were asked to drop to a lower dose if a higher dose made them feel bad, and to only go beyond two doses of 1300 mg per day if they were feeling totally fine. We also asked people never to go above 1300 mg in a single dose or 5200 mg in a day.
Given this protocol, it’s natural that some people ended up on higher doses than others. Here’s the distribution of average daily doses for people who made it the full four weeks:
As you can see, there is considerable variation.
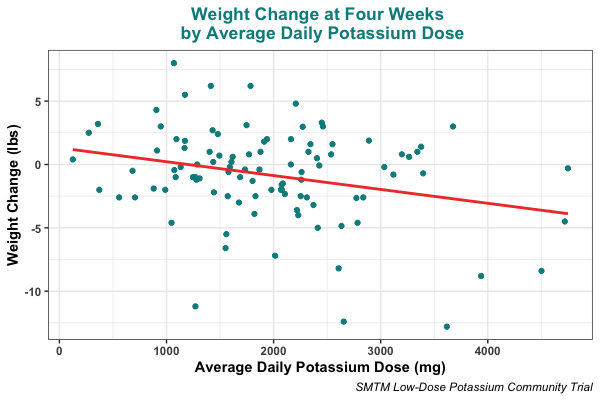
With this information, we can compare the amount of potassium people were taking to the amount of weight they lost. When we do, we see a clear relationship, where people who took more potassium lost more weight on average:
This relationship is statistically significant, r = -0.276, p = .005. This is not an experimental result, since we didn’t assign people to different doses, so we shouldn’t assume it’s causal. There are certainly alternative explanations. For example, there may be weird selection issues. People who chose to take more potassium could have been the people who were like “I feel fine, I’ll take more” or people who were like “It’s not working, I’ll take more” or people who were like “I’m losing a little bit of weight, so I’ll take more and lose more”. But this result is also consistent with what we would expect if potassium supplementation was causing the weight loss.
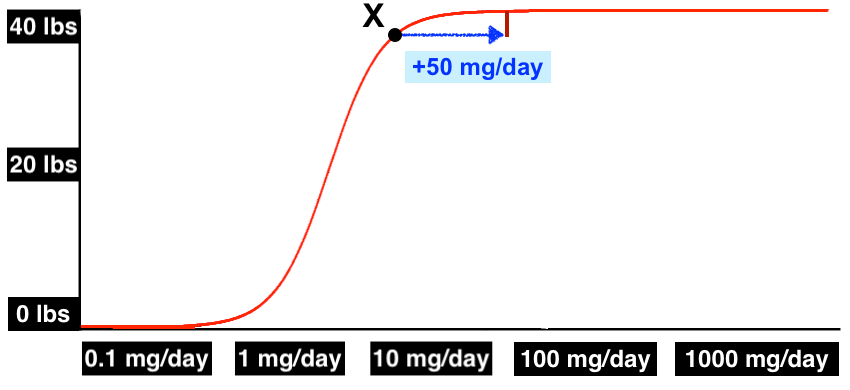
Let’s stop a minute and take a closer look. The regression line here is y = -0.0011x + 1.3110. Essentially what this means is that the model says that on average you would gain 1.3110 lbs if you supplemented no potassium at all for 29 days, but you lose 0.0011 lbs for every mg per day you supplement above that baseline.
For example, someone consuming 2000 mg per day would lose 2.2 lbs more than baseline; since baseline is 1.3 lbs gained, we would expect them to lose about 0.9 lbs on average over 29 days.
The potato diet gives exceptionally high doses of potassium. Sources differ on exact numbers, but the USDA says that a medium potato has about 900 mg of potassium and about 160 calories, so 2000 calories of potatoes a day would give a daily dose of about 11,000 mg potassium.
Plugging that dose into the linear equation above, the predicted weight loss on the potato diet (i.e. on a dose of 11,000 mg/day) would be:
Realistically, the fact that the linear equation in this case lines up with the potato diet so well is just an amusing coincidence. The 95% confidence interval on the slope is [-0.0019 to -0.0003], so model fits for 11,000 mg/day include anything from 19.6 lbs to 2.0 lbs lost.
But you have to agree, it is amusing.
This is in fact moderate support for the idea that potassium is the only active ingredient in the potato diet. We say moderate because it’s certainly not conclusive, but it would be hard for the data to be any more consistent with that interpretation.
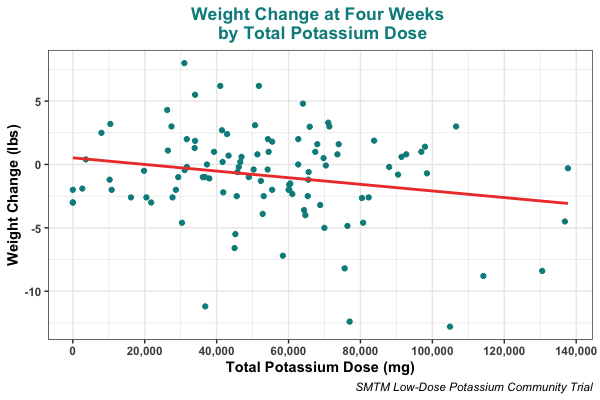
Another interesting comparison can be found in the relationship between weight loss and total potassium taken over the course of 29 days:
This relationship is also significant (r = -0.209, p = .033), though it’s somewhat smaller than the relationship between weight loss and daily average potassium. This may mean that taking a consistent dose is more important than the amount of potassium you take overall, though the confidence intervals of the two correlations clearly overlap, so don’t conclude too much from this difference.
Other than starting BMI and potassium dosage, we can’t really tell why some people lost more weight than others. Sex, reported hormone profile, age, ethnicity, previous experience with the potato diet — none of them seem to matter.
We asked people to report how often they ate meat, eggs, dairy, leafy greens, and tomato products, and while there are sometimes vague trends, none of these variables are ever significantly associated with weight loss. On the other hand, we should note that these were measured in a very rough fashion (just “did you eat it or didn’t you” for each day), so the variables aren’t sensitive enough to detect anything less than a very strong effect.
We also tried looking at all these variables while controlling for starting BMI and daily average dose, but there still don’t seem to be any associations with these variables and weight loss (though it’s possible we’re missing something.)
Similarly, we looked at the variables from the followup survey, but with the exception of one appetite result we will report below, we didn’t find any associations with these variables and weight loss. Even if there were relationships, we probably wouldn’t find them in these data, because there wasn’t much variation in these variables — most participants took potassium in about the same ways and (per our request) didn’t change their diet or exercise during the trial.
So much for absolute weight loss. But what about relative weight loss? Were there signs that the potassium made it easier to lose weight?
Indeed there were, at least in the self-report data. Some people mentioned being surprised at how easy it was to lose weight, and some people mentioned that they were surprised they didn’t gain weight given how poorly they were eating:
(77174810) First of all – holy shit! It’s amazing how well this worked and it’s also surprising that it’s never really been studied before! Thank you for the analysis and thought that you put into this. For this trial, I basically just ate whatever I felt like, went to a football tailgate party nearly every weekend with lots of beer and foods you would not associate with dieting… and still lost nearly 10 lbs! I plan to continue on for at least another couple months so feel free to follow up later if you want to.
…
I have tried every diet/exercise and variation of CICO, atkins, keto, IF, etc., etc., etc. to try and lose weight. To no one’s surprise, nothing really worked for long and the weight always came back. At the end of 2020 I was over 275. It took me three months of busting my ass to lose 20 pounds and as soon as I started eating “normally” again, I slowly started putting weight back on.
(23881640) I started a quick calorie-restricted diet before the holidays (got to fit into those festive pants!), and I’m combining counting macros, counting calories, AND adding 1 tsp of potassium chloride a day to my water, and the weight is coming off. It’s making the calorie restriction much more bearable. I can tell I’m technically hungry, but adherence is so much easier doing it this way. (I lost 20 pounds before by counting macros, and that was hard.)
(60114890) Trial was very easy. Lost 5.5 lbs.
…
I definitely attempted to run a calorie deficit. So, this was a deliberate weight loss attempt. I’ve lost the same 5-15 lbs. maybe six times over the last 30 years. This was the first time it wasn’t really painful and didn’t require a lot of discipline. It’s also the fastest rate of weight loss I’ve experienced (1.5-2 lbs/week as opposed to 0.75-1.0 lbs/week). Very very easy. Why? Mostly appetite suppression. Historically I have been able to run 500 kcal deficits with a lot of effort. I was able to run 750-1000 kcal deficits with almost no effort. Real appetite suppression kicked in after second week, at levels of about 1800mg additional potassium. It was ridiculous—yesterday I ate 1300 kcal and burned 2600 kcal and wasn’t really hungry.
…for my purposes, I don’t really care if its placebo. My appetite was substantially suppressed. It was easy to run a 750kcal deficit. I’m going to stay on the diet until I’m at target weight of 185lbs, which would be total loss of 13.6 lbs. Feels very doable.
This wasn’t a universal experience, but we think these reports were interesting.
It seems possible that for most people, small doses of potassium aren’t enough to cause weight loss by themselves, even if they affect your appetite (see below). But they might still be helpful because they enhance other weight-loss approaches.
At this point we would like to draw your attention to the beverages known as “ketoade” and “snake juice”.
It’s possible that the keto diet works but is hard to stick to, and that ketoade has become popular because it makes weight loss on a restrictive diet much faster and easier. It’s also possible that the keto diet doesn’t cause weight loss at all, and that most successes on the keto diet actually come from people who are taking large amounts of potassium “on the side” as ketoade.
Snake juice is a term for (you guessed it) home-made electrolyte drinks people sometimes take as part of various weight loss strategies, including intermittent fasting, keto, and something called the… snake diet. As far as we can tell, no snakes were harmed in the making of this diet — it appears to refer to how snakes go a long time between meals, since it’s a weight loss strategy about going a long time between meals.
Anyways, snake juice involves drinking a concoction that gives you several thousand milligrams of potassium every day. See this helpful instructional video to learn more. It opens with a man yelling “hey FATTY, behold!” at you, so you just know it is a trustworthy and authoritative source.
In any case, most participants in the potassium trial were essentially drinking ketoade / snake juice / whatever you want to call it: potassium salt and sodium salt mixed in some beverage, often with a little bit of flavoring. And while the effect size was small, on average it seemed to cause weight loss, even without keto or fasting or anything else.
The results of this study suggest that the ketogenic diet community, and this community of “snake people”, have correctly developed a folk wisdom tradition of taking large doses of potassium to amplify their weight loss routines. If so, that is pretty wild, and it speaks well of the value of folk wisdom in solving people’s real problems.
It’s especially interesting that their theories of obesity don’t seem to point at potassium at all. These people don’t think that potassium is the active ingredient here, and they don’t have any idea why potassium might help them lose weight, but they have figured out that they should take it. That’s pretty impressive.
The inverse is true as well. The fact that internet people have settled on potassium salt as part of their folk weight loss routines supports our finding that straight potassium causes weight loss.
6. Effects Other Than Weight Loss
People mentioned a wide variety of effects, but most effects were only mentioned once or twice. One person said that the potassium made their tinnitus worse, but there doesn’t seem to be any sign of this generalizing to other participants.
We did let people report some bonus variables, but most of these variables didn’t get many responses, so we often didn’t end up with a big enough sample size to analyze. For example, only one person reported their total cholesterol on day 29, and no one reported HDL cholesterol, LDL cholesterol, or triglycerides on day 29. So we won’t be taking a closer look at any of those.
Even so, a few things did come through. Here are the effects that people mentioned more than a couple times in the self-report data, or where there were enough measurements to make taking a look worthwhile:
Appetite
The most commonly mentioned effect of potassium was reduced appetite.
(36100230) I found that my appetite was dulled a bit — My mind focused on food a bit less, I snacked less between meals, and ate slightly smaller servings. I found this started to wane a little bit towards the end of the month — not entirely, but I found myself more likely to feel hungry between meals.
(58007117) Taking the potassium was very easy (with the exception of the few times I put nu-salt into pill casings and took it that way – this caused stomach pain, which I did not experience when just taking it dissolved in liquid). My overall impression is that potassium acts as a mild appetite suppressant.
(11538897) I didn’t think of food while doing the trial. At the lower doses, my hunger was affected but my appetite was not. At the higher doses, both were affected. … There was a huge difference in my general desire for food if I took the supplement in the morning before eating. If I took my first dose with food, I would be thinking about food sooner (though I wouldn’t say it was even hunger, just craving). When I took only the supplement and then went to work, it was almost always that I wouldn’t think of food until after work.
(77174810) I settled on 3 doses of ~990mg (3/8 teaspoon) a day at 0730, 1130, 1600. I felt like this kept hunger at the lowest level overall and was easy to stick with. I found that if I took the supplement when I was already hungry, I’d eat more overall. So I take the dose an hour or so before I’d normally eat a meal.
(19620767) Finished the trial. It was weird, I lost a pound the first day, then nothing for a week, then 4 more pounds, then nothing. My appetite was pretty suppressed the whole time, but due to injury and illness I wasn’t really able to exercise beyond going on walks and doing my PT, I also ate an unusually large amount of junk food for life reasons (depression, birthday cake, etc) without gaining any weight.
(18556224) The potassium didn’t magically decrease the calories I took in — I had to consciously restrict them, or have circumstances dictate that — but it did suppress my hunger, i.e. four weeks I was as hungry during the day (mostly not at all) no matter how much food I had eaten.
I haven’t decided whether the weird feeling that potassium gives me is better or worse than the hunger I’d otherwise experience, since I’ve gotten fairly good at handling that.
I haven’t noticed any cravings during the trial, which is good because that is often a problem for me — not craving things carby things, but craving certain foods I eat anyway (butter, cheese) so that I eat more calories than needed, even though I’m not really hungry for anything, just seeking pleasure.
(49045265) I did notice an reduced appetite. There was only one day during the study I was hungry.
(60114890) I definitely attempted to run a calorie deficit. So, this was a deliberate weight loss attempt. I’ve lost the same 5-15 lbs. maybe six times over the last 30 years. This was the first time it wasn’t really painful and didn’t require a lot of discipline. It’s also the fastest rate of weight loss I’ve experienced (1.5-2 lbs/week as opposed to 0.75-1.0 lbs/week). Very very easy. Why? Mostly appetite suppression. Historically I have been able to run 500 kcal deficits with a lot of effort. I was able to run 750-1000 kcal deficits with almost no effort. Real appetite suppression kicked in after second week, at levels of about 1800mg additional potassium. It was ridiculous—yesterday I ate 1300 kcal and burned 2600 kcal and wasn’t really hungry. …for my purposes, I don’t really care if its placebo. My appetite was substantially suppressed. It was easy to run a 750kcal deficit.
(06769604) My appetite was clearly suppressed, especially in the morning. The issue seemed to be that it would come roaring back in the afternoon and I’d be quite hungry.
This was true even for many people who didn’t lose weight, or who lost only negligible amounts. But it wasn’t universal, and some people explicitly mentioned that there was no change in their appetite.
We found this interesting, so we included a question about appetite changes in the followup survey. In these data, the majority of people reported no change to their appetite, but about a third reported decreased appetite, and six people reported greatly decreased appetite. Only one person reported any amount of increased appetite.
And you probably won’t be surprised to see that reduction in appetite was associated with weight loss:
When we treated this self-report measure as a continuous variable on a 1-5 scale, the relationship was significant, r = 0.295, p = .011. But you’ll also notice that many people who did not lose any weight still reported a reduced appetite, suggesting the potassium had some effect for them, just not enough to cause weight loss.
You might think that potassium caused weight loss because it reduced appetite, which caused people to eat less, which caused weight loss. That may be the case, and several people did mention that they were running a calorie deficit. But we also included a field for people to track their calories if they wanted to, and while only 22 people provided complete data, the correlation in that data is nonsignificant and pretty flat, r = -0.100, p = .659.
You’ll also notice that it’s trending in the “wrong direction”, where people who reported eating more also lost more weight.
We don’t think it’s helpful to conclude that potassium is “just an appetite suppressant”. Clearly it is an appetite suppressant, but like, um, why? Why would it do this? Everything has a mechanism. What is the mechanism for this?
We think potassium reduces appetite because it turns down your lipostat. As we said with the potato diet,
[Reduced appetite] is NOT an explanation any more than “the bullet” is a good explanation for “who killed the mayor?” Something about the potato diet lowered people’s lipostat set point, which reduced their appetite, which yes made them eat fewer calories, which was part of what led them to lose weight. Yes, “fewer kcal/day” is somewhere in the causal chain. No, it is not an explanation.
Also not shown: increased body temperature, reduced fat storage, etc.
But even if we accept that potassium turns down your lipostat, you still have to ask, why does it do THAT? What is the mechanism that makes potassium turn down your lipostat’s set point? Well, more discussion in a minute.
Sleep
Some people mentioned noticeable improvements to their sleep.
(24646801) Regarding sleep, in the month or two prior to the study, I had started to wake semi-regularly (5-6 nights/week & 1-2 times per night) to use the toilet. This tapered off rather quickly during the trial and with few exceptions has not returned. I don’t know enough medically to explain why this would be, but it’s definitely an improvement to my sleep, and I would continue the trial indefinitely to retain this result.
(81847724) Sleep is highly subjective but overall I think my sleep quality improved during the experiment, generally sleeping longer without waking up in the middle of the night.
(87352273) Sleep was the most pleasant surprise. I have issues with insomnia, so I tend to stay awake until 2-3 am when I get really sleepy so I don’t end up just lying awake in bed getting frustrated. With ~2000 mg of potassium as well as magnesium before bed, I found myself naturally getting sleepy and falling asleep around midnight every night without much effort or thinking about it.
We included some bonus variables about sleep in the spreadsheet, but the results are inconclusive.
Sleep quality did go up by 0.2 points, but that was not significant (p = .480).
Hours slept went down somewhat, which is interesting, but that change also was not significant (p = .296).
We should note that most people did not report either sleep variable, so the sample size in both of these cases is less than 40. It looks like potassium may improve your sleep a little and/or may help you sleep less, but this isn’t well-supported and even if there is an effect, the effect is probably small.
This is interesting given that Gwern, who is notorious for his attention to detail, did a self-experiment with potassium citrate and “confirmed large negative effects on my sleep”, with a large apparent effect (d = 1.1). Possible differences may come from the fact that Gwern was originally taking potassium in the evening rather than in the morning, and when he tested this he found a difference; was taking about 4000 mg a day, much higher than most people in this trial; and that he was taking potassium citrate, while most people on this trial were taking potassium chloride. (Also Gwern may just be built different.)
Energy
We didn’t find any effect of fidgeting (if anything, people fidgeted less over time), but there were a few self-reports of intense or manic energy.
(87352273) I had really noticeably elevated energy at first, and pretty regularly had the urge to walk or exercise just to burn off some of the nervous energy. The intensity leveled off after the first week or so, but energy overall stayed higher than usual.
(84130320) I had a huge rush of energy, like borderline hypomanic, and I ended up pulling a chest muscle doing pushups because I felt like I was 10 years younger (note to others: you are not actually 10 years younger, do not suddenly do a bunch of pushups). So that sucked.
(93059017) I had so much energy after work that I just needed to walk and I walked an extra mile home.
The participant who lost the most weight (81847724) was also notable for this report:
My mood and energy have been nothing short of fantastic. On a normal day pre-trial, I’d rate my average mood and energy levels in the 4/5 area on the 1-7 scale. Somewhere during week 2 of the trial, I really noticed how elevated I felt in my mood all day long and generally my energy levels were high regardless of the amount of sleep.
However, this increased energy did not seem to be widespread, and some people specifically mentioned not feeling any more energetic.
Looking at the self-report question we included about energy (though FWIW, a sample size of only 29), people’s energy improved by 0.54 points on a 7-point scale, but this was not significant (p = .126).
Surprisingly, Stimulants
A couple people noted stimulant-like effects, and strangely, some also mentioned a kind of stimulant reduction or substitution effect.
(36100230) I felt a little more focused after taking the potassium. A few times I wanted to get some caffeine, and took potassium instead, and no longer needed the caffeine.
(72706884) My caffeine intake decreased substantially during the early part of the diet. I typically intake 100-250mg of caffeine daily. This was reduced to 30-60mg every other day during the first 2 weeks. I found supplementing with a 200mg caffeine pill helpful and used one daily during weeks 3 and 4.
(64983306) While taking potassium, I also experienced heightened concentration abilities, as if I was taking ritalin/adderall. This feeling would last for 2-3 hours after taking a dose of potassium.
We can corroborate this with our own experience. Caffeine seemed to have less of an effect for us while on the potassium, and weirdly, seems to have less of an effect still! Not sure what’s up with that.
Blood Pressure
Only seven people reported their blood pressure readings on day 29, so there wasn’t enough data to do a proper analysis.
However, most of them saw their blood pressure go down, so we figured we should go into some detail anyways.
In the seven cases that reported their BP on both day 1 and day 29, people saw their blood pressure go from:
120/81 to 113/77
114/64 to 116/63
121/91 to 114/78.5
123/90 to 123/80
131/78 to 130/85
111/75 to 99/82
121/78 to 126/81
On average, systolic BP went down by 2.9 points, with a maximum of 12 points down; and diastolic BP went down by 1.5 points, with a maximum of 12.5 points down.
Again, these differences are not significant. But with the very small number of people reporting BP, the sample size isn’t large enough to reach statistical significance. Most of these people also had relatively low blood pressure to begin with, so it’s not clear what kind of change you might see if you had hypertension.
Enjoyment
People were split on the potassium. Many people found it distasteful, and some people hated it.
(50612600) this is way too disgusting to drink
unbelievable it’s sold as a food product
(79606462) it truly does taste horrible, even dissolved in 12 oz water
Unsurprisingly, many of these people chose to end the trial early, and we can’t blame them.
(02689028) does liking kcl salt too much count as anything important
(84130320) My experience overall was actually very pleasant. I didn’t think the taste of the KCl was nearly as bad as advertised. To me, it tasted like salt, if salt were perishable and had spent a little bit too long in the refrigerator. Putting it in sparkling water was fairly good, I could tell it was weirdly salty (especially once I got up to 1300mg/dose) but if I just chugged a little, like half a glass, and then topped it back up it was legitimately delicious. If I did a schorle (fruit juice mixed with sparkling water) instead I could barely taste it. … when I felt really bad and backed off of the potassium per the instructions, I craved potassium. Like I really wanted to eat bananas and was like “boy I could really go for some sparkling water with KCl in it.” It was super strange.
(23578149) I went from finding Nu-Sal revolting (even mixed 2:1 with salt) to finding it pleasant.
But one thing is for sure: it really makes you pee.
(7619655) Have you ever eaten a really salty meal, like pizza or Chinese food, and then felt really thirsty afterwards? That’s how the potassium made me feel a lot of the time. It was drink, pee, drink, pee, drink, pee all day. If I didn’t keep up on the drinking, I would get parched lips and a headache. It was hard to keep this up, so I skipped a bunch of days towards the end.
(74537321) I found I had to pee a lot more often depending on how much water I was drinking. I tried to drink a lot of water throughout the day so I could get the most out of my bowel movements, but one issue was I just had to go pee a lot more. It felt like I would drink a cup of water, and then 20 mins later have to pee like I hadn’t gone all day. 🙂 I would say I had 1 to 2 liters of water per day in addition to meal time drinks (milk, juice, diet soda).
We found these self-reports interesting (also hilarious) so in the followup survey, we explicitly asked people how much they enjoyed the potassium. Because some people mentioned that their opinion of the potassium changed over time, we asked them how they felt about it at both the beginning and at the end of the trial:
In the beginning, most people found it unpleasant or disgusting (though you will notice there is still one “very delicious” rating!), but:
By the end, a majority found it either neutral or pleasant, though many people still found it super gross.
You might expect that potassium enjoyment would be related to weight loss, but we didn’t find much evidence for that. We didn’t notice any statistically significant relationships with weight loss, though looking at the plots does seem suggestive:
So it’s possible that people who enjoy potassium salts are more likely to lose weight by eating them, but if so, the effect is probably too small to detect in this study.
7. Interpretation
The lithium hypothesis is the only theory of obesity that predicts that straight potassium might help people lose weight. It’s not a very strong prediction, we simply noticed that lithium and potassium are both monovalent cations, and that they appear to have some interaction in the brain, where the lipostat is located. But other theories wouldn’t predict a relationship between potassium and weight loss at all.
We first introduced the lithium hypothesis in Part VII of our series A Chemical Hunger, expanding on the idea in Interlude G, Interlude H, and Interlude I. In Part X, the conclusion to the series, we speculated that if obesity is caused by lithium exposure, potassium might be an effective treatment:
Lithium … is an alkali metal ion that appears to affect the brain. Other alkali metal ions like sodium and potassium also play an important role in the brain, and there’s evidence that these ions may compete with each other, or at least interact, in interesting ways (see also here, here, and here). If lithium causes obesity, it may do so by messing with sodium or potassium signaling (or maybe calcium) in the brain, so changing the amount of these ions you consume, or their ratios, might help stop it.
However, the results of this study are not conclusive evidence in favor of the lithium hypothesis, and it benefits us to explore some alternative explanations.
Prosaic explanations like “potassium caused people to lose water weight” would seem to be ruled out by the fact that many people’s appetites got noticeably weaker, and the fact that some people mentioned that they had never lost weight so quickly or easily before. Same thing for placebo.
So the two classes of likely alternatives are that either it’s something confounded with the potassium dose (i.e. when you take more potassium, you also do more X), or that potassium causes weight loss for some other reason than its relationship to lithium.
Deficiency
A natural starting point is to consider whether obesity could be just another disease of deficiency, one you develop if you don’t get enough potassium. Scurvy is the disease that happens when you don’t get enough vitamin C, beriberi is the disease that happens when you don’t get enough vitamin B1, could obesity be as simple as a potassium deficiency?
Unfortunately we think that is not the case. Diseases of deficiency are easy to identify because they regularly crop up in situations where people eat a limited diet for a long time. Both beriberi and scurvy, for example, were common among sailors on long voyages.
Obesity does not really fit this profile. People today may not be getting enough potassium, but if obesity were a disease of deficiency, you would expect to see it showing up in historical records of cities under long sieges, sailors on long voyages, explorers in the Antarctic, and so on.
We see two distant ways to reconcile this idea, however. The first would be if potassium deficiency causes obesity, but only over the very long term. For example, maybe you only develop obesity if you eat a low-potassium diet for 10 years. This would be unusual and we think it is unlikely, but it’s consistent with the data.
The other is if obesity occurs in the rare cases when people both have a potassium deficiency AND have lots of access to calories. Sailors, explorers, and other people who tend to get diseases of deficiency usually are not eating that well in general. Maybe obesity is only triggered when you’re not getting enough potassium, but you can otherwise eat as much as you want. We think this also seems unlikely, but again, we can’t rule it out.
Hydration / Clearance
People drank a lot more water on the potassium trial because the potassium salt made them thirsty, and they had to pee a lot. People also drank a lot of water on the potato diet, for similar reasons. Is it possible that both diets cause weight loss because they encourage you to drink huge amounts of water, and that water flushes your system (or something)?
This seems pretty unlikely to us, though it is consistent with all the evidence. If someone wants to try the super-hydration community trial, where you try to drink 5 liters a day or something (don’t use that number we made it up, figure out what is actually safe), that would be fairly interesting. We don’t expect it would cause comparable weight loss, in part because we think someone would have noticed by now if staying hydrated was enough to cure obesity. But it sure would be interesting if it did!
Sodium
Potassium and sodium balance each other in biological functions. To regulate the increased amount of potassium they were consuming, we encouraged people to consume more sodium as well, and they may also have naturally craved more sodium as they ate more potassium.
As a result, people on the potassium trial may have been getting more sodium than normal. For similar reasons, people on the potato diet may have been getting more sodium than normal. So one kind of weird possibility is that sodium is what’s causing the weight loss here, not potassium.
We did have this in mind from the start, so one of the bonus variables for the study was estimated daily sodium intake.
Unfortunately, out of the 233 people who entered data, only 20 people tracked their sodium, so we don’t have much evidence. But what evidence we do have doesn’t support this interpretation. People who consumed more sodium actually ended up with higher weights at the end (r = 0.101), though the relationship is not significant (p = .670).
In general we do not expect that sodium is responsible for the weight loss observed in this study, nor would we encourage anyone to try a high-sodium diet. But again, we can’t really rule it out.
Other Biology
Is it possible that potassium increases the clearance of something other than lithium? Just making more urine will increase the clearance of some things! Or could it treat obesity in some other way?
It seems likely, but we can’t really be much more specific than that. Potassium has approximately one zillion roles in biology, so for example if obesity is caused by anything to do with “hormone secretion and action”, which seems like a pretty broad category, potassium could potentially be a treatment. This seems like a question for someone who knows more about biochemistry than we do.
8. Future Studies
There are a number of studies that could be run to get more information. We might run some of them ourselves in the future. For now, here they are as brief sketches.
Experimental Extensions
We know that one of the biggest criticisms we’re going to get on this study is about the lack of blinding and lack of a control group. Everyone in this study took potassium, and everyone knew exactly what they were taking.
Let’s imagine what a control group might look like. It’s well-established that people get heavier as they get older, so over the course of 29 days, people who do nothing should on average end up weighing slightly more by the end. We’re pretty sure that a straight control group would have lost about 0 lbs and maybe would have gained some small fraction of a pound over the course of the study — if you gain 2 lbs a year, that’s about 0.17 lbs a month.
But it’s true that people in this study were paying more attention to their weight and to their diet, and it’s possible if they were taking packets of some other white powder that wasn’t potassium, they would lose weight for some other reason. It’s possible that there’s some level of placebo.
That’s fine, because this study was never intended to be the final word. It’s the first study, not the last.
While the hierarchy of evidence is very important, a meta-analysis of multiple randomized controlled trials doesn’t just happen overnight. With this study, we’ve shown that it’s plausible that potassium by itself could lead to weight loss. There wasn’t evidence for that before.
For example, this comment from the extremely measured thread by Agaricus
But now that we have this evidence, it might be worth investing more time and energy in a more controlled or more complex study.
We wouldn’t want to do a straight control group where people do nothing, because that would reduce our effective sample size and it would be boring for participants. Fortunately, there are designs that can help with both problems. Here are two ideas:
First of all, we could run a crossover trial. In this case, the study would run for two months. One half of the participants would be assigned to take potassium for the first month and then take no potassium for the second month. The other half of the participants would be assigned to take no potassium for the first month, and yes potassium for the second month. This allows both groups to serve as controls without reducing our sample size.
Another idea would be to run a dose-dependent experiment. The design might look something like this: one half of the participants would be assigned to a protocol that involves them working up to a dose of 2000 mg of potassium a day. The other half of the participants would be assigned to a protocol that involves them working up to a dose of 4000 mg of potassium a day. (You could also do a dose-dependent experiment with more conditions — some people assigned to 1000 mg a day, some to 2000 mg/day, some to 3000 mg/day, etc.) If potassium is the active ingredient, you should see more weight loss in the group(s) assigned to the higher dose(s).
Comparing different doses allows us to have a control group without having to have a “no treatment” group that spends the month doing nothing. Both groups are providing valuable data, and we still control for the effect of the intervention. It isn’t blinded, but this design guards against placebo effects because it would be hard for the people in the 4000 mg/day group to arrange to lose more weight than the 2000 mg/day group.
The main issue in both cases is statistical power. You might need very large sample sizes to detect these differences, and no one should run one of these studies without conducting a very careful power analysis. But, the designs are theoretically sound.
Other Diet(s) High in Potassium
Potatoes are very high in potassium, but they are not the only food that is very high in potassium. Other foods that are very high in potassium include lima beans, swiss chard, spinach, bamboo shoots, butternut squash, kohlrabi, portabella mushrooms, white beans, bok choy, and many others (though avocado and banana are maybe overrated as sources of potassium!).
If the potato diet causes weight loss because it’s high in potassium, a non-potato diet that is high in potassium might also cause weight loss. So one thing you could do is arrange a trial of some other high-potassium diet and see if that also caused weight loss.
This isn’t a sure thing, however. Other foods do contain potassium, but it’s possible that the potassium is different in these other foods — less bioavailable, released more slowly, part of a different compound, etc. So we don’t think this would be a very strong test of the theory, because it introduces so many new variables.
In addition, we want to note that many of the items on the list of high-potassium foods are foods that we suspect might be high in lithium. In particular, there’s evidence that lithium accumulates in leafy greens, sprouts, and maybe in gourds, which matches most of the foods on the list above. If the potato diet works because it’s high in potassium AND low in lithium, these other high-potassium foods might not have any effect at all.
If we had to pick just one high-K food to test, we would probably pick coconut water. It’s a liquid, so the potassium is probably more available than average. It’s relatively high in potassium, with about 600 mg per cup. It’s easy to find and requires no preparation. And (as far as we know at least) coconut water isn’t swimming with lithium. So if people wanted to try getting 2000+ mg per day of potassium from coconut water, that would be pretty interesting.
Low-Potassium Potato Diet
In the course of designing this study, we came across a set of practices used to remove potassium from potatoes. Some people with serious kidney disease have to avoid consuming too much potassium, and these techniques were developed so they could enjoy potatoes safely. Potassium removal is usually accomplished by slicing or dicing the potatoes in small pieces to increase surface area, and then soaking (before and/or after cooking) or boiling them in water to leach out the potassium (e.g.: link, link). Some sources claim that this can remove more than 50% or even up to 70% of the potassium in potatoes.
We could test these techniques by preparing some potatoes with these methods and sending the potatoes (and the water they were soaked/boiled in, which should contain the removed potassium) to a lab for analysis. If the sliced/boiled/soaked potatoes had much less potassium than potatoes that were baked or roasted or something, that would suggest that these techniques remove potassium as advertised.
We could then use this information to do another test of the weight-loss powers of potassium, by running an experiment with a modified form of the potato diet.
One group would be assigned to eat a potato diet with potatoes prepared in a way that preservesas much potassium as possible (probably baked), and the other group would be assigned to eat a potato diet with potatoes prepared in a way that removesas much potassium as possible (probably boiled and then soaked and then fried). If the preserves-potassium group lost a lot more weight on their potato diet than the removes-potassium group, that would be further strong evidence that potassium is the main active ingredient in the potato diet.
This prediction matches the following tidbit from M’s experience with the potatoes-by-default diet, which makes it seem somewhat more more plausible: “I seemed to be able to eat much more when the potatoes were sliced/grated (e.g. Swiss rosti, Chinese tudousi) than when they were closer to whole potatoes (i.e. diced, potato wedges, etc.). I’m not sure why.”
Some people think that the potato diet works because it is a mono diet. It cuts out most other foods, so there’s very little variety, and some people (e.g. here) think that food variety is part of what makes people gain weight. But if soaking all the potassium out of potatoes made for a much smaller effect, that would mean there was a big difference in weight loss between two otherwise-identical mono diets, which would be hard for food variety to explain.
Potato Diet with Urine Test
One plausible hypothesis is that potassium helps clear lithium from your brain, and this is why it causes weight loss.
If this were the case, most of the lithium that is cleared from the brain should end up in your urine (urinary lithium seems to be a good proxy for levels in the body in general). It should be possible to test people’s urine for a while to establish a baseline, and then start them on the potato diet and see what happens. The level of potassium in their urine should increase dramatically, since there is so much potassium in potatoes. It would be interesting to see if the level of lithium in their urine increased as well.
If urinary potassium levels were correlated with weight loss, that would be more evidence that potassium is the active ingredient (though they might not be correlated, since urinary potassium levels are part of a control system). If urinary potassium levels were correlated with urinary lithium levels, that would be more evidence that potassium is forcing lithium out of your brain (or some other reservoir). And if urinary lithium levels were correlated with weight loss (or frankly, even if they just went up when you started the potato diet), that would be strong evidence in favor of the idea that lithium is the cause of the obesity epidemic.
This could be the smoking gun for the lithium hypothesis, which makes it a pretty attractive idea. The problem is that we don’t have any experience running studies with urine samples, so we’re not sure how to design this study or how to run it. We’re also not sure whether it’s possible to run it over the internet, or if we would have to get a bunch of people together in person. If you do have experience in running studies with urine samples, and you’re interested in helping, please contact us.
However, even this study might not be conclusive. It’s possible that potassium counteracts the effects of lithium but doesn’t increase the rate of clearance. For example, potassium might compete with lithium in the brain without forcing it out. It might reduce lithium absorption in the small intestine. It might keep lithium from leaching out of your bones. It might do something else. (Lithium pharmacodynamics remain poorly understood.) So while it’s plausible that potassium increases lithium clearance, we aren’t confident that’s how things work.
9. Conclusion
We ran this study because we suspected that potassium might be the active ingredient in the potato diet, that the high levels of potassium found in potatoes might be why a diet high in potatoes causes weight loss. These results support that interpretation.
The weight loss observed in this trial was small on average, but the doses of potassium were intentionally very low. There’s evidence that the relationship between weight loss and potassium consumption is dose-dependent, such that people who took larger doses lost more weight on average. Regression modeling suggests that someone who was consuming a dose of potassium equal to the amount provided by the potato diet would lose a similar amount of weight as people lost on the potato diet.
These results are not decisive. Indeed, no results ever are. However, given the small doses involved, the results could not be more strongly consistent with the potassium hypothesis.
Potassium supplementation is scientifically valuable because it’s relatively controlled. But it’s not very practical, because it’s not clear if large doses of straight potassium salt are safe for most people, and because many people find potassium salt really gross. We strongly recommend that anyone who wants to lose weight should do the potato diet instead. The potato diet gives a much higher effective dose of potassium while probably being a lot safer, and may have other benefits.
The all-potato diet is a relatively big commitment (though much easier than most people expect), so you may prefer to try the half-tato diet instead. This involves getting about 50% of your calories from potatoes and, based on the available case studies, seems to be more than 50% as effective and much less annoying. We plan to study it more soon.
If for some reason the potato diet doesn’t work, we would recommend you try to find some other way to eat a diet that’s exceptionally high in potassium.
If none of these things work for you, then you can try direct potassium supplementation, though you should consult with your doctor, definitely not do it if you have diabetes or kidney disease of any kind, and limit yourself to no more than 5000 mg a day.
We probably will not follow up on this study at 6 months and 1 year, since the average weight loss was so small. It seems unlikely that 0.89 lbs of weight loss will be statistically detectable several months later.
However, several people reported that they are planning to stay on the potassium longer-term, so we may have more results soon from the people who reach 60 days on low-dose potassium.
If you would like to be notified of future stupid studies, or if you want to keep up with our work in general, you can subscribe to the blog by email (below), or follow us on twitter.
And if you feel like reading this post has added a couple of dollars’ worth of value to your life, or if you have lost weight as the result of our research and you think it improves the quality of your life by more than one dollar a month, consider donating $1 a month on Patreon.
Thanks for going on this journey with us.
Sincerely, Your friendly neighborhood mad scientists, SLIME MOLD TIME MOLD
APPENDIX A: Delivery
People overwhelmingly took potassium chloride (93.3%), overwhelmingly as a salt (92.3%), and mostly as the brand Nu-Salt (62.9%). The most popular method of delivery was to take it dissolved in water, juice, a sports drink, or some other beverage.
We didn’t detect any differences in weight loss for any of these variables, but given that almost everyone took the same kind of potassium in roughly the same way, we wouldn’t have the statistical power to detect any differences unless they were really huge. So there may be differences, but we wouldn’t expect to see any evidence for them in this data, and indeed we do not.
However, the delivery method does seem to make a difference in terms of enjoyment. Here is a sample of people’s recommendations:
(45454797) The metallic taste went away after just a few days and I found the salt to actually taste good with a little apple cider vinegar and water. Gatorade without the sugar! (and easier than pressing lemons all the time)
(40941749) I highly recommend orange fanta if you’re gonna drink your magic potion, and hash browns if you wanna eat it.
(77174810) Yes, KCl tastes gross/weird/bad. I tried a few different concentrations and mixtures with food (don’t mix with a bite of guacamole – yuck!). What I discovered was that mixing it with Simply Strawberry Lemonade makes it very palatable! I dissolved the KCl and a little sea-salt in about 1 oz of water. Then added about 4-6 oz strawberry lemonade. You could damn near sip it this way! Apple cider was the second best mixer.
(94352426) Higher concentrations were only drinkable to me in carbonated drinks made it okay to drink. For me this was the biggest limiting factor, always having to have carbonated water in home, buying it every time I went grocery shopping those bottles are a lot of extra weight.
Though there was considerable variation:
(52533228) By far, the easiest way for me to integrate it into my routine was to add it as a salt substitute in my cooking or meal prep. I could not stand adding it to drinks – the taste was usually awful and harsh. When it was added to food, the flavors mixed well in general and it was much much less noticeable.
(79332762) In terms of taking the potassium, I really disliked it. I would happily take a pill 1-2x per day, but I really dislike the taste of KCL. I tried two approaches to taking it, mustard & lemonade. With mustard it worked ok for low doses (1/8 tsp) but for larger doses it felt like too much salt hitting my stomach at once. With lemonade I don’t want to routinely drink enough lemonade that fully masks the flavor. I also really like lemonade as a treat so making it a daily routine (& making it taste bad) felt weird. I don’t really want to chug powerade/gatorade either.
APPENDIX B: Regulated Success
The body puts in a lot of effort to make sure you don’t get too much potassium. So one thing you might expect to see on this trial is that people start losing weight at first, but as their body acclimates to the extra potassium and their kidneys start filtering it out more aggressively, they stop losing weight and they maybe even gain back the weight that they lost.
Some people did mention something along these lines. For example, participant 98856740 (who submitted after Dec 1 and whose comments are therefore not in the main dataset):
I lost 6 pounds in the first week and then didn’t lose any more. In fact I bounced between that low number and about three pounds higher. During that weight loss period, I felt hot, enough to wake me up at night. I’ve heard people describe hot flashes during menopause that way. Once I got to the plateau stage, I no longer felt hot, just normal. I speculate that my metabolism was using heat to lose weight. I have no idea why it stopped. I don’t think there was anything materially different about the early days.
From the data, we’re not sure what to think. On the one hand, there are very few clear reversals. For example, the number of people who dropped 5 lbs at some point but ended up losing no more than one pound by day 29 is two, specifically these two participants:
But on the other hand, most people hit their minimum weight well before the last week of the study, suggesting that many people hit a plateau early on. Here’s the plot where we highlight each person’s day of minimum weight:
You can see that some people did hit a relatively low minimum weight early on and then never go down further from there. This may be evidence that some people hit a plateau.
APPENDIX C: Accounts of Greatest Weight Loss
81847724
Well, my time in the experiment has been shocking, to say the least of it. So obviously I’m morbidly obese so I should probably address that right away considering I’ve lost over 12 lbs during this experiment.
In January 2022, I started working with a doctor that specializes in weight loss. I was put on a low-carb, ketogenic diet 6 days per week with 1 day of free eating anything I wanted, and an exercise routine of moderate walking every other day. My starting weight was ~485 lbs. My compliance with the diet and exercise routine was 100% from January until the start of the potassium trial. My starting weight at the beginning of the trial was 476.2 lbs, so I lost approximately 9 lbs during that 9-month time frame.
I DID NOT change my diet or exercise habits during the trial to any appreciable measure. There were a couple of times I mixed up my exercise routine but mostly I stuck to the same 60 minutes on a treadmill every other day. Any changes to the exercise were noted in the sheet.
Overall I think it’s incredible that the simple change of adding potassium seems to be responsible for a sudden change in the rate at which I was able to lose weight. I will be continuing supplementing potassium going forward, this is the single most amount of progress I’ve made in weight loss in a month.
I’m going to try to think of anything I can disclose here to give context to the data.
Potassium was consumed from Nu-salt and mixed with a Gatorade zero powder that also had some potassium (both details recorded on the sheet). I didn’t have any set schedule for the potassium, I simply added it whenever I felt thirsty and acquired water (up to the dose limit for the day)
My diet was a strict ketogenic diet (under 20 grams total carbohydrates per day, gross carbs, not net) for 6 days per week and one day a week of eating anything I wanted. I do not track calories. I don’t track macros other than the number of carbohydrates consumed to stay under 20. The 20-carb limit includes the 2g carb per serving of the Gatorade zero powder I used to mix the nu-salt.
I weighed myself completely naked on an “Ideaworks JB5824 Extra Wide Talking Scale” between 8:30 and 9:00 AM every day, preferably after having a morning bowel movement. If I didn’t have one, I would still record my weight. I made a note on the sheet whether or not I had a bowel movement for that particular day.
My heart rate was tracked using an AmazFit band with the pulse check feature, typically immediately before or immediately after weighing myself in the mornings.
Sleep is highly subjective but overall I think my sleep quality improved during the experiment, generally sleeping longer without waking up in the middle of the night.
My mood and energy have been nothing short of fantastic. On a normal day pre-trial, I’d rate my average mood and energy levels in the 4/5 area on the 1-7 scale. Somewhere during week 2 of the trial, I really noticed how elevated I felt in my mood all day long and generally my energy levels were high regardless of the amount of sleep.
During the first week of the experiment I remembered to measure my waist circumference as per the CDC method but frankly, I forgot to do that, but I have included a final measurement.
A final note about compounding factors: lithium reduction
I first discovered Slime Mold Time Mold through the “A Chemical Hunger” series of blog posts, but in particular, the section covering lithium is what caught my attention for potential causes of obesity. The reason it caught my attention is I was put on lithium to treat a neurological condition that I was diagnosed with (tourette’s syndrome) when I was 7 years old, and I can positively say that was the time when I began to put on weight steadily over years and decades regardless of my diet and exercise habits. I am 36 years old and have been off lithium for over 10 years now, but the lithium article really resonated with me as a potential cause. So I’ve installed activated carbon and reverse osmosis water filtration systems on all of the water taps in my house since the first lithium post in 2021. The filters I’m using the claim to remove “over 90%” of lithium from water. (City of Cincinnati water, Cincinnati, OH)
So I don’t know how entirely relevant all that could be to the data, but all of the water that I was mixing the potassium in was also water being treated for the removal of lithium specifically (although its been approximately a year of running filtered taps and only the addition of the potassium has resulted in dramatic weight loss)
I did not participate in the potato diet trial.
Anyone that wants to supplement potassium with Nu-salt should try mixing it with the Gatorade zero powder, it almost completely covers the taste and made the trial a breeze.
One last thing, I chose to limit the amount of Nu-salt I was consuming at the 1300mg per serving mark just because I didn’t want to go through my supply of Nu-salt and Gatorade zero powder too quickly. I felt entirely fine with the amount I was consuming and believe I could have easily continued in either increasing to higher doses or adding more 1300mg doses throughout the day.
Well, I feel like I’m rambling at this point but if there are any questions please feel free to ask, in the meantime I’m going to continue supplementing with potassium.
74537321
First I just wanted to clarify that I have been following a Time Restricted Eating, or Intermittent Fasting plan since Sep 30th, prior to learning about this study. I was excited to join the study since I found your posts on Twitter talking about the potato diet that people have raved about. I’ve been eating my meals between 12pm and 6pm every day and I’m sure it has contributed significantly to my weight loss. I hope this doesn’t skew the study results too much as a result of my eating schedule.
I did focus on keeping my calories under 3000 per day with a target of 2500. I also made an effort to exercise 2 to 3 times per week of 30 mins or more. That being said, I do think the potassium helped me manage my hunger, and specifically I felt like I didn’t need to eat that much during the day to feel full.
I found the study relatively easy to do. I set reminders for each dose through out the day, as well as a reminder for recording my weight and waist measurements and used an app to track those using my smart scale and smart measuring tape, both from Renpho. I discovered that drinking each dose with straight water was the easiest and fastest way to get it down. I tried with other drinks and things, but I just knew going in that it would taste funny, and got it over with quickly each time.
Starting out I didn’t have an 1/8th teaspoon measure, so I just started with 1/4 teaspoon. Being 6’4″ and 300 lbs, I figured I could handle a larger dose to begin with. Then as a result of not paying attention to the instructions very well, I ended up going up pretty quickly in dosage the first two weeks. For side effects, it was noticeable the first few days where I felt some stomach discomfort, and general unease, but it went away after the first week. The only other side effect that I think was related to the potassium, is that I found I had to pee a lot more often depending on how much water I was drinking. I tried to drink a lot of water throughout the day so I could get the most out of my bowel movements, but one issue was I just had to go pee a lot more. It felt like I would drink a cup of water, and then 20 mins later have to pee like I hadn’t gone all day. 🙂 I would say I had 1 to 2 liters of water per day in addition to meal time drinks (milk, juice, diet soda). I’m going to continue my eating and exercise schedule, but will stop taking potassium and just record my stats each day for the next month. I’d like to really see how the weight loss was impacted by the potassium. I’ll keep updating the spreadsheet and see how things go. I’m happy to talk more about my experience or answer any questions as part of any follow-up.
58007117
My 4 weeks are done, although I intend to keep taking potassium given the moderate success I experienced. Taking the potassium was very easy (with the exception of the few times I put nu-salt into pill casings and took it that way – this caused stomach pain, which I did not experience when just taking it dissolved in liquid). My overall impression is that potassium acts as a mild appetite suppressant. Thanks for running this trial, I’m looking forward to reading about the compiled results.
01538897
Sorry for the delay- I couldn’t load the sheets properly on my phone, but I was keeping track and am just now getting the chance to fill out the last week. Please excuse the order of the train-of-thought below.
I took my last weight the morning of Thanksgiving and proceeded to eat my weight in food. I haven’t been eating fast food lately but the cravings hit me hard (probably from a combination of eating way too much, alcohol, and not supplementing for a couple of days). My plan for now is to finish up leftovers today, grab some fast food over the next couple of days, and probably restart a 30 day period on Wednesday having gained about 5 pounds in a week.
All of my supplementary data (heart rate, sleep, exercise) was from my fitbit.
It was very true that I didn’t think of food while doing the trial. At the lower doses, my hunger was affected but my appetite was not. At the higher doses, both were affected.
The biggest struggle for me was trying to keep track of my calories. I feel like it negatively impacted my trial because it did affect what I ate, even though I was supposed to eat whatever I wanted. I would eat what I wanted and feel shame/guilt for eating over X amount of calories (arbitrary number from back in my restriction days). The perhaps more interesting way it affected the trial was, once my appetite started being affected by supplementing, I would finish meals that I wouldn’t have because “I had already tracked the calories for it, I should get it,” “how can I track 1/3 of a meal,” etc. For my second attempt at the trial I will not be tracking calories, and hopefully not have the pressure of numbers to affect my eating habits. I understand that it was an optional variable anyways, but hypothetically the change in weight would reflect the appx input anyways.
I did not look into the lithium correlation at all, but if it is important- for meat markers, I only eat white meat. For egg markers, I only eat egg whites. The only thing I noticed that seemed to give me actual hunger pangs was if I drank a significant (about or more than 24 oz in a sitting) diet soda. Of course you can see in my data that alcohol also ruined a couple of days, but that didn’t actually make me feel any more hungry, just more crave-y and less likely to resist eating an entire pizza (apparently).
My work schedule is Fri/Sat nights, Sun-Tues mornings, and a random overtime on either Wed or Thur. Although my Fri shift is the same every week, there is a huge difference between that 3pm-11pm shift and my Tues 530-130 shift in terms of when and what I typically eat (and my sleep schedule).
There was a huge difference in my general desire for food if I took the supplement in the morning before eating. If I took my first dose with food, I would be thinking about food sooner (though I wouldn’t say it was every hunger, just craving). When I took only the supplement and then went to work, it was almost always that I wouldn’t think of food until after work. If I took a dose without food and then went on my walk, even if I had already eaten that day, I would feel very light-headed.
I’m happy I found out about this trial. I am generally pleased with the outcome, if not the methods I specifically used, and am more excited about starting next week with a little less restriction. I’ll still track in case the data is useful for you, but probably only the weight and doses.
98295681
[SMTM’s note: despite the comment below, this participant reported losing 8.6 lbs.]
Thanks for running this trial, it was interesting. My subjective feeling is that the potassium supplementation had no discernable effect on my brain function, hunger/diet, or weight. I’m planning to continue supplementing potassium though because my food diary shows my intake of it was very low and I’m curious whether it might have any longer term effects past just the first 4 weeks.
77174810
First of all – holy shit! It’s amazing how well this worked and it’s also surprising that it’s never really been studied before! Thank you for the analysis and thought that you put into this. For this trial, I basically just ate whatever I felt like, went to a football tailgate party nearly every weekend with lots of beer and foods you would not associate with dieting… and still lost nearly 10 lbs! I plan to continue on for at least another couple months so feel free to follow up later if you want to.
Interestingly, I was born and raised in Colorado. I lived there for my first 30 years until 2003 when we moved to the East coast and although I am a bigger person (6’5″/225 in 2003), I was never really “heavy” until maybe 2010 or so. I kept putting on weight as I aged into and past my 30s and I just followed conventional “wisdom” that it was due to getting older. Each year I would have a few extra pounds.
I have tried every diet/exercise and variation of CICO, atkins, keto, IF, etc., etc., etc. to try and lose weight. To no one’s surprise, nothing really worked for long and the weight always came back. At the end of 2020 I was over 275. It took me three months of busting my ass to lose 20 pounds and as soon as I started eating “normally” again, I slowly started putting weight back on.
Anyway, you may have just solved obesity. I hope you enjoy being billionaires. Don’t forget us little guys that did nothing but participate in your study when you are trying to decide on the color for your private jet (I think dark blue would be nice).
Notes and observations:
Yes, KCl tastes gross/weird/bad. I tried a few different concentrations and mixtures with food (don’t mix with a bite of guacamole – yuck!). What I discovered was that mixing it with Simply Strawberry Lemonade makes it very palatable! I dissolved the KCl and a little sea-salt in about 1 oz of water. Then added about 4-6 oz strawberry lemonade. You could damn near sip it this way! Apple cider was the second best mixer.
I felt thirsty a LOT of the time, especially in the first week or so. I increased my water consumption by over a quart/day for the duration of the study (still ongoing)
On the weekends, I ate poorly (nutrition wise) but still overall was eating way less than I usually did.
I only tried a 1320mg dose once. I didn’t feel great but cannot say for sure that it was that higher dose. I plan to try two higher doses/day for the second month
I settled on 3 doses of ~990mg (3/8 teaspoon) a day at 0730, 1130, 1600. I felt like this kept hunger at the lowest level overall and was easy to stick with.
I found that if I took the supplement when I was already hungry, I’d eat more overall. So I take the dose an hour or so before I’d normally eat a meal.
I’m very curious about this mechanism for weight loss. Does K+ just act as an appetite suppressant? Or is it more that the lipostat is turned down and that makes you less hungry? If lithium passes through the body fairly rapidly, how long does the effect last on the brain (if that is what is happening)? When I have cut calories in the past, it was an uphill battle to fight hunger. Presumably my lipostat was set too high so I’d be hungry and also not lose weight effectively because my body was not trying to lose weight. Hmm, might make sense… I plan to do this for at least another month if not two. It will be interesting to find out:
Could there be any detrimental long-term effects of taking this much extra K?
If I stopped the supplemental K, will I start to trend back up in weight? How hard will it be to keep the weight off?
How long does the effect last? Will I be (normal) hungry tomorrow if I stop supplements today?
I intend to experiment with the following after I hit my target:
Could I take the supplement every other day or once a week as a “maintenance” dose and keep the weight off? Or maybe just a smaller daily dose? Looking forward to your further analysis and trial results.
The email has been lightly edited for clarity and to help preserve anonymity, but otherwise what appears below is a faithful reprinting of the original report as we received it.
Hello Slimes (Slime?),
I’m very excited to write to you. In some ways it is weird that you are the last to hear about my experience with the potato diet, since roughly everyone in my life has probably heard more potato-talk than they’d ever really want.
Starting in July, I ate “potatoes by default”, which is to say if I didn’t have anything better to eat, I’d eat potatoes. This meant that if I had plans for lunch or dinner, I would eat whatever it was I would’ve normally eaten ad libitum, and I tried actively to prevent the diet from materially interfering with my lifestyle (I drank alcohol socially as I normally would’ve, I participated in all the meals I normally would’ve participated in with friends, I tried arbitrary new dishes at restaurants, etc.).
I started doing this because I was very intrigued by the reports of the changes to the psychological sensation of hunger in your study. I’ve always seen hunger as a psychologically weird thing. For example, I would often find myself physically extremely full to the point of discomfort, but would still want to eat more, especially if there was still food in front of me (often is not anywhere close to every day or every week, but frequently enough that this is an experience I feel pretty well-acquainted with). I would also tend to get super hungry around 5pm each day and couldn’t stop thinking about what I was going to have for dinner. I was also happy to lose some weight, but I value social life and food experiences pretty highly, and did not want any diet to interfere with these aspects of my life.
In practice, “potatoes by default” meant I was eating potatoes for roughly 1/3 of my meals, mostly for lunch when I was working from home during the week or on weekends, since I usually had dinner plans of some kind. My preferred preparation was to air-fry diced potatoes (unpeeled, though I’d typically use Yukon gold potatoes which have thin skins) tossed in some combination of {salt, soy sauce, pepper, dashi broth, herbs/spices, gochujang paste}, which I found to be both very tasty and time-efficient (~5 min of prep time and ~20 min in the air fryer). I would usually eat about 1 pounds of potatoes in a single sitting. I did experiment with a bunch of other preparations, and probably the most interesting thing I noticed here was that I seemed to be able to eat much more when the potatoes were sliced/grated (e.g. Swiss rosti, Chinese tudousi) than when they were closer to whole potatoes (i.e. diced, potato wedges, etc.). I’m not sure why.
I tossed my diced potatoes in olive oil before air frying, and more generally used olive oil, duck fat and avocado oil to cook other potato preparations. I probably used 1-2 “glugs” of oil per 1-1.5lb potatoes across these preparations (“lightly greased”, call it). And of course in my non-potato meals, I consumed whatever oil – and other ingredients – restaurants would be using to cook their food. Given my diet was substantially made up of non-potato meals that I actively tried to keep “as before”, I think it is a safe bet that there wasn’t any particular type of food (diary, oil, red meat, etc.) I stopped consuming, or even materially reduced my consumption in, as a result of potatoes by default (beyond the generic ~1/3 reduction from swapping out a third of my meals to be mostly potato). FWIW, I tend to have low belief in hypotheses like “zero of X is special”; in general, I’d expect the difference in response between “zero” and “some” of any given input to be closer to continuous than discrete in the setting of a complex system like the one we’re thinking about.
The most succinct way to summarize the experience is probably with the below set of charts, which I had actually shared as part of a talk I gave at my fiancee’s company about potatoes and your work on obesity (I did say people around me have heard a lot about potatoes). The right chart is just a zoomed-in version of the left chart. The vertical red line is when I began the potato diet and the gray bars are when I was traveling / ate no potatoes. I plotted the results of your study in orange to compare; my version of the diet seems to be strictly less effective, but not by much I think. I wonder if the orange line (100% potato) would just hit the plateau faster, or if it would reach a different stabilized endpoint.
I think my main reaction to the data was that it was kind of insane? I was eating potatoes a third of the time and literally whatever else I wanted the rest of the time, and losing weight almost as quickly as the full potato diet. The gray bars (cumulatively more than a month) appear to make no dent in the overall trend, especially the first two bars when the weight loss was most rapid. Potatoes just seem unreasonably effective.
While charts are often worth many words, I think the qualitative commentary around the experience is probably just as interesting:
Early on, maybe a two or three weeks in, for the first time in a really long time, I did not have the urge to finish off leftover food at dinner. That was a big “wow, what is going on” moment.
The second gray travel bar was me traveling through Singapore and Bali. I’m a big fan of food, and was excited to try different hawker stands, etc. But I found my appetite was significantly diminished and I couldn’t try as much food as I wanted to. This was particularly striking since I was not eating potatoes at all in this period – there seems to be something more going on than just the “mechanical” effect of having potatoes in your belly (although I do believe high satiety per calorie is an important but incomplete part of the story; I think it’s unlikely that I’d consume much more than ~1000 calories/day if I was only eating potatoes, on the sole basis of how satiating they are).
The third gray travel bar (the past week) was me spending time at my fiancee’s parents house for Thanksgiving. As a good future son-in-law, I basically just ate as much as they wanted to feed me, and of course it was a lot. So this was the first time during the course of the potato diet where I ate to the point of discomfort. Juxtaposed against the past couple of months, I was able to notice a very distinct difference in the sensation of full-ness here, which I think I can only describe as “physically full, but not spiritually full”. My stomach was mechanically full of food, but it was almost a completely different sensation of full-ness (and one that felt much “emptier”) than I’d have after eating a lot of potatoes.
It’s been 4.5 months since starting potatoes by default, but I spent five weeks of those 4.5 months traveling / not eating potatoes. Conditional on not traveling, I think I ate potatoes for 1/3 on my meals (maybe more like 50% early on, and more like 20% more recently), but that means overall, I was really eating potatoes for only 25% of my meals on average in this period.
After ~3 months, I went to my doctor to just make sure I was healthy, given the rapid and material weight loss I had been experiencing. He gave me a blood test for CBCD, CMP, a lipid panel, and HgbA1c, and apparently everything was fine (I have no idea what these tests are so just reporting them).
I was extremely aggressive about cutting out eyes and sprouts in my potatoes when preparing them. I basically figured it was extremely costly to get sick of potatoes (or live in fear of eating a chunk of potato that tasted gross) if my goal was to eat potatoes long-term, and potatoes are very cheap from a $ perspective. So I’d strongly recommend anyone considering a long-term potato diet to do the same.
I tended to keep skins on since I think they are good for fiber intake. But I find it harder to do this with thick-skinned potatoes like Russets. I have no issues at all with thin-skinned potatoes like Yukon gold.
I was mostly not worried about nutrition, getting enough protein, etc., since the majority/supermajority of my meals were regular food.
I play squash once or twice a week, and didn’t notice anything difference in my ability here.
I didn’t experience a feeling of increased energy as some others reported.
Given my experience, it seems like there is roughly no reason to go anywhere close to full potato. Just on priors, it seems kind of unlikely moving a relatively small portion of your diet to a single food would have any adverse health effects or other effects, and it seems you get pretty close to the benefits of full potato (though as noted above this depends a bit on whether the full potato diet gets you to the same plateau point faster, or gets you to a different plateau point).
I am planning on more or less just continuing to eat potatoes by default, possibly forever? There’s basically just no downside for me to do so, beyond the ~30 min of prep work I have to do to make potatoes (instead of say, ordering delivery as I normally would).
So, that’s the summary of the last 4.5 months of my life. My friends/coworkers have bought into potatoes to varying degrees, from simply no longer avoiding potatoes, to a friend participating in your KCl study. I hosted a Potato Con at my apartment a few weeks ago; we had 10+ unique potato dishes and a great turnout. I’m guessing as a fraction of my personality, potatoes will begin to fall off going forward, but as above, I expect as a fraction of my diet, they will continue to be a meaningful presence.
Thanks for all the super interesting research you guys have been doing on this. I read A Chemical Hunger at the start of July (two weeks before starting the potato diet), and found it incredibly compelling and well-researched. I don’t know if lithium is the thing, but the environmental contaminants hypothesis seems pretty hard to argue against. Keep up the great work, and let me know if there’s anything else I can tell you about my experience or otherwise to be helpful.
Jeff Nobbs and Zero Acre Farms released a white paper titled How Vegetable Oil Makes Us Fat, which is partially a response to the questions we raised in response to Nobbs’ previous work in Interlude E: Bad Seeds of A Chemical Hunger. We’ve read the new piece and are going to discuss it with Jeff and the rest of his team, and we’ll put out more posts if the discussion changes our mind about the role of vegetable oils in the obesity epidemic.
Do children prefer candy or potatoes? It’s not the most rigorous experiment of all time, but this informal halloween study by @jana_pruden suggests that many if not most children prefer the potato (as do 77% of twitter respondents). Someone should do a replication, maybe next halloween?
Hacker News comment claiming that it is 100x brighter outside than inside. “I bring this up because one of the largest factors in myopia development appears to be outdoor light exposure in childhood.”
If you’re worried about the death of twitter, why not move to Twitter 2, a Google form and Google doc maintained by a math professor at the University of Toronto.
Simon Sarris on twitter argues that B12 deficiency is common, and may be the cause of what is often diagnosed as anxiety, executive dysfunction, depression, and even autism. If he’s right, this would be pretty easy to study and would be an amazing finding. We haven’t gotten a chance to take a close look yet, curious to know if people think this theory is plausible.
@CollinLysford shares an interesting test from @qkate that claims to reliably distinguish between chronic fatigue and depression. Ask your patient, “if you felt completely better tomorrow, what would you do?” If they go, “idk”, it’s depression. If they describe a huge list of things they would love to pursue, it’s chronic fatigue. Whether or not this test actually works for depression vs. CFS, Collin is entirely right that this is the kind of “ontological firepower” we need more of.
Command+F to search documents for text strings has changed scholarship. Tools like this OpenAI API from Dwarkesh Patel will change it even more.
Dapplegrim is a Norwegian fairy tale collected by Peter Christen Asbjørnsen and Jørgen Moe in their Norske Folkeeventyr. A man comes home to find that his parents are dead and his elder brothers have split up the family fortune — all he’s inherited are 12 mares, each of which has just had a foal. He praises the most beautiful foal, which tells him he should kill all the other foals and let it drink the milk of all 12 mares for a year. The young man is like “sure sounds reasonable” (“Yes, the lad was ready to do that; so he killed all those twelve foals, and went home again”), kills the other foals, and comes back a year later to find the foal “so fat and sleek, that the sun shone from its coat”. Events escalate to the point where the man and the giant horse go to hell and kidnap the Devil’s horse to win the hand of the princess in marriage.
Nicky Case is doing an unofficial Potato Diet 3-Month Follow-Up Survey, at that link. Nicky is doing this because she’s “too impatient for the 6-month follow-up, and also because a 6-month follow-up wouldn’t be able to tell the difference between ‘weight regained at fast as the original weight loss’, and ‘weight regained at 1/6 the rate as the original weight loss’.” If you participated in the potato diet and you’re interested, consider filling it out!
Paper from 2020: negative association between percentage of obese people and water hardness in water purification plants (in Japan, which may not be all that representative.) The correlation is about r = 0.5, but the sample size is only 9 regions. The paper says this is statistically significant but unless we’re missing something, r = 0.5 shouldn’t be significant with n = 9. So probably don’t take this one too seriously but still, food for thought.
Dana Fischer “is an American Magic: The Gathering player. She is tied for the youngest to make the second day of a Grand Prix tournament (at age eight) and is the youngest to win cash at a Grand Prix (at age nine). … Her father started teaching both daughters Magic when they were very young, before they could read the card text. They learned to play by memorizing the cards. … After they learned to read, the process went faster.” Inevitable comparison to the Polgár Sisters.
Friend of the blog @atroyn is starting a new grant program: “if you sleep on a mattress on the floor anywhere in the bay area, if accepted someone will come to your house and install a bed frame” (actually by this point applications are closed)
Living plant controls a machete through an industrial robot arm. “Plant machete has a control system that reads and utilizes the electrical noises found in a live philodendron. The system uses an open source micro-controller connected to the plant to read varying resistance signals across the plant’s leaves.”
*Poem by One Named Huie from Heungshan Encouraging the Traveler*
Just talk about going to the land of the Flowery Flag and my countenance fills with happiness. Not without hard work were one thousand pieces of gold dug up and gathered together. There were words of farewell to the parents, but the throat choked up first. There were many feelings, many tears flowing face to face, when parting with the wife. Waves big as mountains often astonished this traveler. With laws harsh as tigers, I had a taste of all the barbarities. Do not forget this day when you land ashore. Push yourself ahead and do not be lazy or idle.
Drugs have effects. Take more of a drug, and you’ll get more and bigger effects. They call this a dose-response relationship — take some dose, get some response. Benadryl makes you drowsy, mercury gives you hallucinations, cyanide kills you.
But these effects only kick in above certain doses. At very low doses, the drug has no effects. This always has to be true, because at zero dose, the drug can’t have any effects.
Then at some dose, the effect starts kicking in. Sometimes this means you start feeling it a little and it gets stronger over time. Other times, it means the response rate increases, and more people start feeling the effect as they take bigger doses.
At some point, the effect is as strong as it can possibly get and it doesn’t get any stronger. Everyone who is going to have a reaction is getting the strongest effect they can get.
Dose-response relationships can be described with dose-response curves, like this one:
Often these curves make the most sense on a log scale (probably because this is bounded exponential growth; it’s exponential but eventually everyone who is going to have the effect already has it), so for this exercise, we’ll be portraying the x-axis on a log scale. This may not be true for all drugs, but it’s a reasonable starting place.
Lithium is a metal that is also a drug that sometimes causes weight gain. But no one really knows what the dose-response curve for weight gain on lithium looks like. Weight gain is clearly a side effect of clinical doses of lithium (about 50-300 mg of elemental lithium a day), at least for some people. But almost no one has studied lithium doses below 50 mg a day, so we don’t know at what point this weight gain effect starts kicking in.
The dose-response curve could look like this, where weight gain doesn’t show up until you hit therapeutic doses of 100 mg/day and more:
The y-axis is 0 to 40 lbs, this is arbitrary, graphs are for illustration purposes, not real data, etc.
Or it could look like this, where effects kick in starting at subclinical doses of as low as 1 mg/day:
Or it could even look like this, where weight gain starts at trace doses of less than 1 mg/day, and once you’re getting 10 mg/day, you’re maxed out:
The curve could be spread out, with gradual effects increasing across all plausible doses:
Or it could be incredibly abrupt, where weight gain happens suddenly once you’ve passed a certain threshold:
There’s also good reason to believe the dose-response curve will be different for different people. The response may be different in terms of the shape of the curve, when the effects kick in, and when they max out.
By ancient tradition, we will call our example patients “Alice” and “Bob”. In this hypothetical, Bob starts seeing weight gain as he approaches 1 mg/day and has already gained almost 40 lbs at 10 mg/day, but Alice doesn’t get the same effects until noticeably higher doses:
It might also be different in terms of the maximum effect. In this next example, not only does Alice not start gaining weight until 10 mg/kg, she caps out her weight gain at just over 20 lbs, while Bob gains 40 lbs on a similar dose:
Psychiatric doses of lithium are in the 50-300 mg range (elemental), and some people think this means that weight gain must happen in this range. But this may not be the case.
First of all, there’s plenty of evidence suggesting that the psychiatric effects of lithium kick in at trace doses of less than 1 mg/day. The effects may not be very strong at trace doses, but you can still pick them out in a population-level analysis. In fact, there’s a wholedangliterature finding that rates of dementia, suicide, homicide, and other “behavioral outcomes” are associated with trace lithium levels in drinking water. This suggests that some effects kick in at very small doses.
But regardless of whether or not trace amounts of lithium lower the suicide rate, the fact is that lithium has several different effects, and there’s no reason those effects can’t kick in at different doses. It might look something like this:
In this case the y-axis is in percent, not lbs, since you can’t have pounds brain fog.
(To be clear, all these curves are completely made up for the purposes of illustration.)
This should probably be our default assumption. Most drugs have multiple effects, and different effects often kick in at different doses. For example, alcohol is a drug that makes you talkative at low doses and makes you puke your guts out at high doses.
(Your mileage may vary. Adam Mastroianni, who reviewed this piece, says, “Not me, I puke a tiny amount at tiny doses, increasing to a massive amount of puke at large doses.”)
dose-responsefigureshowing different effects
In fact, we know that lithium has effects that kick in at different doses, because therapeutic effects tend to kick in well before patients die from lithium toxicity, and death is also an effect.
It’s true that some people don’t gain weight at all, even on clinical doses of more than 1000 mg/day. But this might just mean that in their case, the dose-response curve for weight gain is above the dose-response curve for toxicity/death. You can’t get there without dying, so we never see it. (And for some people, the mechanism by which lithium causes weight gain probably just doesn’t work at all.)
In any case, we have almost no information about what the curves might look like for lithium, because there’s very little research on doses below the low end of the clinical range (around 50 mg/day). There’s that literature on trace doses in drinking water which we mentioned above, and there’s one RCT from the ‘90s finding that trace doses of lithium made violent offenders friendlier and happier — but as far as we know, there’s never been any formal study on doses in the range of 1-50 mg/day. If anyone has studied weight gain on lithium doses below 50 mg/day, we’ve certainly never seen it.
So let’s see what we can do to figure out anything at all about the dose-response curve for the weight gain effects of lithium — and, maybe more interesting, the effects of lithium in general. Do any of these curves start showing up at subclinical doses?
Nootropics Survey
One thing that’s interesting, in terms of our bigger “is lithium exposure causing the obesity epidemic?” question, is that most of the side effects of lithium are non-specific — if you feel nauseous and tired, it could be lithium exposure, but it could equally be a million other things. That makes it hard to tell if symptoms of lithium exposure have increased over the past 50 years, since no one has been tracking brain fog rates since 1970. If the rate of increased thirst has dectupled, we might not even know (unless…).
Some of the effects we’re going to study — like fatigue, depression, and muscle weakness — are also symptoms of hypothyroidism. These are also nonspecific, but if they were to increase, they might be diagnosed as hypothyroidism. We’re curious to see if they increase on low, subclinical doses.
The survey was pretty straightforward. First, we asked people for their basic demographic information. Then, we asked them to describe their previous experience with lithium.
We allowed people to record information for up to five different doses of lithium — different in either being different amounts (e.g. 1 mg/day vs 5 mg/day), different compounds (e.g. lithium as lithium orotate vs. as lithium carbonate), or both.
For each dose, we asked people to tell us what compound they took, how much they took per day, and approximately how many days they tried the dose for.
We also asked them what effects they experienced on each dose. Our list of effects was based on this page from Mayo Clinic, though our list did not include all the effects mentioned on this page.
We make no claims that our list is any sort of principled selection — it’s just a subset of effects we decided to include. There were too many to include all of them, so we made some calls.
In particular, we focused on “milder” side effects, since we knew that the nootropics folks would be on lower doses than a clinical population and would probably not experience the more severe effects. We also combined some effects to avoid redundancy — for example, we combined multiple effects related to passing gas into the single effect “flatulence” on our list.
We do regret cutting “fruit-like breath odor” and “eyeballs bulge out of the eye sockets”. Now those are side effects.
In any case, the final list was:
Increased clarity / focus
Increased calm
Improved mood
Improved sleep
Trouble sleeping
Weight gain
Weight loss
Confusion, poor memory, or lack of awareness
Fainting
Fast, pounding, or irregular heartbeat or pulse
Frequent urination
Increased thirst
Slow heartbeat
Stiffness of the arms or legs
Troubled breathing (especially during hard work or exercise)
Unusual tiredness or weakness
Brain fog
Dizziness
Eye pain
Headache
Vision problems
Depression
Diarrhea
Drowsiness
Lack of coordination
Loss of appetite
Muscle weakness
Fatigue
Nausea
Ringing in the ears
Slurred speech
Trembling (severe)
Bloating or indigestion
Flatulence
Decreased libido
Loss in sexual ability, desire, drive, or performance
Tooth pain
We also included an option for “other”.
Finally, because we are especially interested in weight changes, we also asked for each dose, “If you lost / gained weight, what was approximately the magnitude of the loss / gain”, with answers in kilograms.
Recruitment
Nootropics enthusiasts often take small amounts of lithium, usually because they believe it has a variety of beneficial effects at low doses, effects including balanced mood and reduced stress. So recruiting from the nootropics subreddit seemed like a good way to find people who already have experience with subclinical doses.
A total of 40 people filled out the survey, providing data on at least one regimented dose (an amount taken daily for a period of time) of lithium. Of these, 20 people also reported on a second dose, 5 reported on a third dose, 2 reported on a fourth dose, and one person reported on a fifth dose. From this we can see that of the respondents, 50% have tried at least two different doses of lithium at some point.
For now, we will ignore that some of these doses are the same people, and just treat these as 68 different individual doses. Going back and doing more complex modeling at some point would be a good idea, we encourage that, but it’s not the focus of the post today. To keep it clear, we will call these “cases”. There are 40 people who gave us 68 cases.
Two people don’t report how much they were taking for their second dose, however, so we will be ignoring these cases. In the end we have 66 cases.
This is all self-report, and we haven’t been at all strict about kicking people out. In fact, we didn’t kick anyone out. Some of the data do look a little strange. One person reported taking 5 mg/day of lithium carbonate, which seems unlikely. But we’re taking the data at face value for now.
Doses
First of all, we want to see how much elemental lithium everyone is taking.
Many people reported a single number for their daily lithium dose, but some people reported a range, e.g. “5mg-20mg”. To convert this into a single number for analysis, whenever a person gave a range of values, we went with the average of the range endpoints. In this example, a report of “5mg-20mg” would be converted to 12.5 mg.
Different lithium compounds contain different amounts of elemental lithium. This is the “active ingredient”, so to speak. We did our best to estimate elemental lithium from the numbers people reported. In most cases, this was pretty straightforward. Lithium carbonate is prescribed by the weight of the compound, and the elemental dose is 18.8% of the weight of the listed dose. Lithium orotate usually lists elemental lithium on the packaging, and so most of the time, no conversion is needed.
However, we did have to guess on a few. For example, one person said that they were taking lithium orotate, but said they were taking 130 mg per day. Based on what we know about lithium orotate doses available on the market (see e.g. here), we think 130 mg elemental is very unlikely — this is probably 5 mg elemental, so we coded it as 5 mg. For all these conversions, you should be able to double-check our numbers in the raw data (available on the OSF).
Having made these conversions, we find that people were taking doses between 0.25 and 282 mg per day elemental lithium, over spans ranging from 1 day to 4 years. We use dose per day because it’s easy to track. Here’s the distribution:
As you can see, most people were taking less than 50 mg/day. In fact, most were taking less than 25 mg/day. The median daily dose in this sample is 10 mg/day, the mean is 39.6 mg/day, and the mode (15 people) is 5 mg/day. The next most popular dose after the mode is actually 1 mg/day — 6 people were trying that amount.
In comparison, the average therapeutic dose is 50-300 mg/day elemental lithium, usually delivered as lithium carbonate. So overall, these nootropics folks are taking rather small doses.
Lithium orotate was by far the most popular compound in our sample. This makes a lot of sense — lithium orotate can be purchased over the counter, or over the internet, without a prescription, and comes in relatively low elemental doses, all of which makes it an ideal nootropic. Of the 66 cases, 42 people were taking lithium orotate, 22 were taking lithium carbonate, and one each were taking lithium aspartate and “Lithium Chloride / Ionic Lithium”.
We keep saying “doses”, but it’s important to keep in mind that from a biological point of view, these are not really doses — these are deltas, a change in the daily dose. People are already getting some small daily dose of lithium every day from their food and water, so whatever they are taking as a nootropic is a dose in addition to the dose they were already getting. We don’t currently know what kinds of doses people are getting from food and water — the literature is a little confused at points — but we’re confident that it’s more than zero.
So while we don’t know if the average American is getting 5 mg/day from their food or just 0.05 mg/day, we know they’re getting some amount — for now, let’s call the average everyday dose X. If someone is taking 5 mg/day as a nootropic, they’re not getting a total dose of 5 mg/day, they’re getting X + 5 mg/day.
Weight Change
Let’s start by looking at weight change on these low doses.
Like the doses themselves, weight change was also reported as a range in a few cases. Like the doses, whenever someone gave a range, we took the mean of that range as our point estimate value.
Here are the weight changes people reported compared to the daily elemental dose they were taking. Note that the weight changes here are in kilograms:
That plot is a little hard to read because most people are taking low doses (< 50 mg/day) so most of the points are crammed in over on the left side. To make it easier to read, here’s the same plot with the x-axis log10 transformed (with some jitter in the x-axis to keep points from overlapping):
One caveat is that these plots include many people who didn’t actually mention any weight change at all. Since they didn’t mention it, we assumed the weight change on their dose was effectively zero. This seems like a pretty safe assumption, but just in case, here’s the same plot with only the people who explicitly said something about their weight change:
Most people didn’t see any weight change, or at least, they didn’t report any. But 8 of the 66 cases did report some weight change.
The first weight change reported is a loss of 3 kg, at a dose of 5 mg/day. This is a low dose, and it’s weight lost, not weight gained, which makes it something of an outlier.
The first weight gain reported is an increase of 5 kg on 20 mg/day, which this participant reported taking for approximately 365 days. The next weight gain is 8 kg on 50 mg/day, which the person reported taking for only 60 days.
After 50 mg, weight gain seems to be more common, though certainly not universal. Of people who took more than 50 mg/day elemental, 6 of 18 reported weight gain, which is 33%. The highest weight gain reported was 35 kg (not pounds, he was quite clear) on 56.4 mg/day elemental taken as 300 mg/day lithium carbonate, over 4 years.
So, keeping the limitations of the small sample in mind, this suggests that the weight gain effects kick in around the range of 20–50 mg/day of elemental lithium, for somewhere in the ballpark of one third of people.
The sample size is quite small, but if you squint, it does kind of look like weight gain kicks in a bit earlier for Lithium Orotate than for Lithium Carbonate. We didn’t expect this, but while we were working on this project, a reader pointed us to a small literature finding that lithium orotate is sometimes effective at a lower dose than lithium carbonate.
This is a literature that currently seems to be driven by Anthony Pacholko and Lane Bekar, two Canadian researchers from Saskatchewan, building off of the work of Hans Nieper in the 1970s. In the interest of full disclosure, we should tell you that Wikipedia describes Nieper as “a controversial German alternative medicine practitioner” whose therapies have “been discredited as ineffective and unsafe.” The “see also” links at the bottom of his page are “List of unproven and disproven cancer treatments” and “Quackery”. Caveat lector.
In any case, there is a review by Pacholko and Bekar from 2021, which does cite many sources outside Nieper, and says in the abstract, “[lithium orotate] is proposed to cross the blood–brain barrier and enter cells more readily than [lithium carbonate], which will theoretically allow for reduced dosage requirements and ameliorated toxicity concerns”. They also have an empirical study published in 2022, which reports benefits of lithium orotate over lithium carbonate in mice.
We’re not going to review the whole literature here, but it’s worth noting. Let’s mark it down for now as suggestive.
Other Effects
Weight gain is not the only effect of lithium. It might not even be the most interesting effect.
The nootropics people on reddit dragged us for mostly including negative effects — which, you know what, totally fair. We should have included more positive effects. We’re interested in seeing when the bad stuff kicks in, but while we were at it, we should have looked at when everything kicked in. If we study this again, we’ll include more positive effects.
We also now realize that we should have asked for the effects on a scale (1-7, 0-3, something like that). Asking just “did you experience increased thirst or not” gives us very little information for most of these symptoms. If we study this again, we’ll use more detailed measures.
But for now, let’s look at the data we have. And the data we have are already pretty interesting. People reported experiencing all sorts of effects:
And, to our surprise, they reported lots of these effects even on pretty low doses:
As before, this is a little hard to read because of the squashing. Here’s the same thing with the x-axis log10 transformed:
Even below 10 mg/day elemental (a 1 on the x-axis above, since this is log10), most people are reporting a few of these effects, and some of them are reporting several. Above 10 mg/day elemental, almost everyone reports multiple effects! It’s clear that stuff starts kicking in at pretty small doses.
Moving beyond the aggregated effects, we can ask, what effects popped up specifically? Here’s the list, with the number of cases that mentioned each effect:
Increased clarity / focus: 14
Increased calm: 38
Improved mood: 35
Improved sleep: 23
Trouble sleeping: 7
Confusion, poor memory, or lack of awareness: 12
Fainting: 0
Fast, pounding, or irregular heartbeat or pulse: 1
Frequent urination: 10
Increased thirst: 11
Slow heartbeat: 0
Stiffness of the arms or legs: 1
Troubled breathing: 2
Unusual tiredness: 5
Brain fog: 13
Dizziness: 5
Eye pain: 2
Headache: 3
Vision problems: 1
Depression: 5
Diarrhea: 4
Drowsiness: 5
Lack of coordination: 4
Loss of appetite: 5
Muscle weakness: 2
Fatigue: 8
Nausea: 2
Ringing in the ears: 3
Slurred speech: 2
Trembling (severe): 3
Bloating or indigestion: 4
Flatulence: 2
Decreased libido: 10
Loss in sexual ability, desire, drive, or performance: 4
Tooth pain: 0
And here are the top 10:
Increased calm: 38
Improved mood: 35
Improved sleep: 23
Increased clarity / focus: 14
Brain fog: 13
Confusion, poor memory, or lack of awareness: 12
Increased thirst: 11
Frequent urination: 10
Decreased libido: 10
Fatigue: 8
We see that the four positive effects are the most commonly reported, which is what we would expect from a population of nootropics users who are taking lithium in search of positive effects. More than half of the cases reported “increased calm” and “improved mood”, and around a third reported “improved sleep”. On top of this, 14 reported “increased clarity / focus”. Of the 66 cases, 50 (about 75%) reported at least one of these four positive effects.
But this also makes it especially striking that so many people reported negative effects. If anything, this population is inclined to downplay the negative effects of lithium, but negative effects were reported quite frequently.
The most commonly reported negative effect was brain fog (13), followed by “confusion, poor memory, or lack of awareness” (12). These sound like the same thing, but there wasn’t perfect overlap. We see that 7 people reported brain fog without reporting confusion, and 6 reported confusion without reporting brain fog.
It’s pretty weird that “increased clarity / focus” is the fourth most common effect and “brain fog” and “confusion, poor memory, or lack of awareness” are effects #5 and #6. Aren’t these polar opposites? Why are they right next to each other in the rankings? Sounds like a possible paradoxical reaction.
The next most common effects were increased thirst (11) and frequent urination (10), which also seem related.
After that, the next most common is decreased libido (10), which is supported by a less common but related effect, “loss in sexual ability, desire, drive, or performance” (4). These are both reported at rather low doses, as low as 1 mg/day.
The next most common are fatigue (8), and trouble sleeping (7), and then we get into numbers too small to go over individually. But even so, almost every symptom we put on our list was reported by at least one person — we certainly did not expect that. The only three symptoms that no one reported were fainting, slow heartbeat, and tooth pain.
Some of these symptoms, like ringing in the ears (3), are only reported by people who were taking more than 50+ mg/day. But lots of effects start appearing at very low doses.
C5H3LiN2O4 , his name is my name too
Like with the weight gain, there might be more effects for orotate than for carbonate at the same elemental dose. Don’t take this as conclusive — there’s not all that much evidence. But it is intriguing.
We can even do a regression looking at just the data from cases where people were taking carbonate or orotate. This brings us to a somewhat unusual finding.
When the dose of elemental lithium is used to predict the total number of lithium effects, the regression model finds significant main effects of both dose (p = .0008) and compound (p = .021), and a significant dose-by-compound interaction (p = .0019). The total R-squared is 0.257, which is pretty good. This model suggests that lithium orotate does bring on more effects at a lower dose than lithium carbonate.
But, there is only a main effect of dose (p = .005) when dose of elemental lithium is log10 transformed. In this case, the compound (p = .899) and the interaction (p = .718) are not significant, though the R-squared is pretty similar (0.245).
This difference is pretty clear when we plot both models with their regression lines. Here’s the situation if you don’t log-transform the daily lithium dose. You can clearly see that the slopes of the two lines are very different:
But here’s the situation if you do log-transform the daily lithium dose. You can clearly see that the slopes of the two lines are nearly identical:
This is a little weird. On the one hand, that’s a pretty clear interaction in the non-transformed data. On the other hand, we would expect log transformation to be the appropriate transformation for this analysis. Make of that what you will.
Troof points out that a lot of this interaction seems to be driven by a single participant, who looks kind of unusual and is taking an unusually high dose of lithium orotate. If you look at the plots, you can see them as a somewhat clear outlier (taking the most orotate and having the most effects of anyone on that compound). So probably don’t put too much trust in this data point, and without it, the case for an interaction basically disappears.
Conclusion
These results suggest that many effects of lithium kick in at subclinical levels. In this sample, the majority of people who took at least 1 mg of elemental lithium a day reported at least one effect, and people on doses above 5 mg/day tended to report experiencing several effects.
The most common effects people reported were the four positive effects we asked about, but several negative effects of lithium were commonly reported as well, especially brain fog, “confusion, poor memory, and lack of awareness”, increased thirst, frequent urination, decreased libido, “loss in sexual ability, desire, drive, or performance”, fatigue, and trouble sleeping. A slight majority of cases (53%) reported at least one negative effect.
Weight gain was not a common effect, but it was reported at relatively low doses. The lowest dose for reported weight gain was on a dose of 20 mg/day, and the next lowest was on 50 mg/day. The greatest reported weight gain was on a dose of only 56.4 mg/day. Taken together, this suggests that in the current environment, lithium can cause noticeable weight gain on elemental doses below 50 mg/day, and possibly as low as 20 mg/day.
Unfortunately, this does not tell us all that much about the dose-response curve. There are just too many degrees of freedom, and we don’t know that X value, the amount that people are getting from their food and water. It could be that X is well below the dose-response curve, and +50 mg/day is needed to push you onto the curve:
But it could equally be the case that X is well onto the curve — past the point of greatest sensitivity! — and a big delta like +50 mg/day is needed just to see any weight change at all.
This evidence doesn’t rule anything in, but it does rule some things out. Given these findings, we can mostly rule out the idea that doses below 10 mg/day have no effects. We can also rule out the idea that weight gain starts kicking in at just 0.1 mg/day — it seems pretty clear that you need a bigger delta than that. But we can also mostly rule out the idea that weight gain only occurs above 600 mg/day.
So while it’s good that some things are ruled out, we still don’t know enough to pin down the dose-response curve.
At least, not for weight gain. We do see what looks like evidence of the dose-response curves for other effects.
Troof also played around with the data a bit, and sent us the following graph. The pattern is clear for some effects and rather messy for others, but we see what looks very clearly like the start of a dose-response curve for increased thirst. We also see what look like dose-response curves for improved mood, improved sleep, increased calm, and increased clarity, where rates of the effects increase and then level off. But there isn’t a clear curve for brain fog or confusion, at least not in these data.
One weird thing we noticed is that most of these dose-response curves come down at the highest dose level, suggesting that some of these effects actually get less likely past a certain point. Not sure what’s going on there, we’re interested to hear what people think.
Human Challenge
At this point you might be wondering: should someone do a human challenge trial for low-dose lithium? You know, round up some brave souls on the internet, get them all to take 10 mg’s worth of lithium orotate every day for a month, and see what happens to them by the end. Is that a good idea?
We don’t think this is a good idea, for a couple reasons. First of all, we don’t know what X is, which means that increasing the dose by a fixed amount isn’t actually all that informative.
Second, we’re pretty sure that X is different in different places and for different people. Combine this with the fact that different people probably have different dose-response curves for strictly genetic reasons, and the results begin seeming hopelessly complicated.
Finally, while low-dose lithium does seem to have positive effects for many people, some of its effects are quite nasty. We wouldn’t want to subject volunteers to unnecessary brain fog and fatigue. If we were sure that the study would teach us a lot, then maybe it would be worth it, maybe we would be open to convincing people to give it a go. Maybe we would try it ourselves. But since we don’t think it would really answer any of our biggest questions, we don’t think a lithium supplementation study would be worth anyone’s while.
However, Troof has convinced us that there are more than 40 people out there who have already tried subclinical doses of lithium, and that at least some of them will be reading this post. So we’ve put together an updated version of our survey that fixes some of the problems we mentioned above — it asks about the magnitude of each effect, includes more positive effects, and includes more effects in general. If you’ve taken lithium before, you can fill out the survey here, and if we get enough responses, we will post another analysis. If you filled out the first survey, you can fill this one out too, because this one is a little more detailed — just check the box that indicates that you took the first survey, so we can make sure not to double-count you.