
[PART I – MYSTERIES]
[PART II – CURRENT THEORIES OF OBESITY ARE INADEQUATE]
[PART III – ENVIRONMENTAL CONTAMINANTS]
[INTERLUDE A – CICO KILLER, QU’EST-CE QUE C’EST?]
[PART IV – CRITERIA]
[PART V – LIVESTOCK ANTIBIOTICS]
[INTERLUDE B – THE NUTRIENT SLUDGE DIET]
[PART VI – PFAS]
[PART VII – LITHIUM]
[INTERLUDE C – HIGHLIGHTS FROM THE REDDIT COMMENTS]
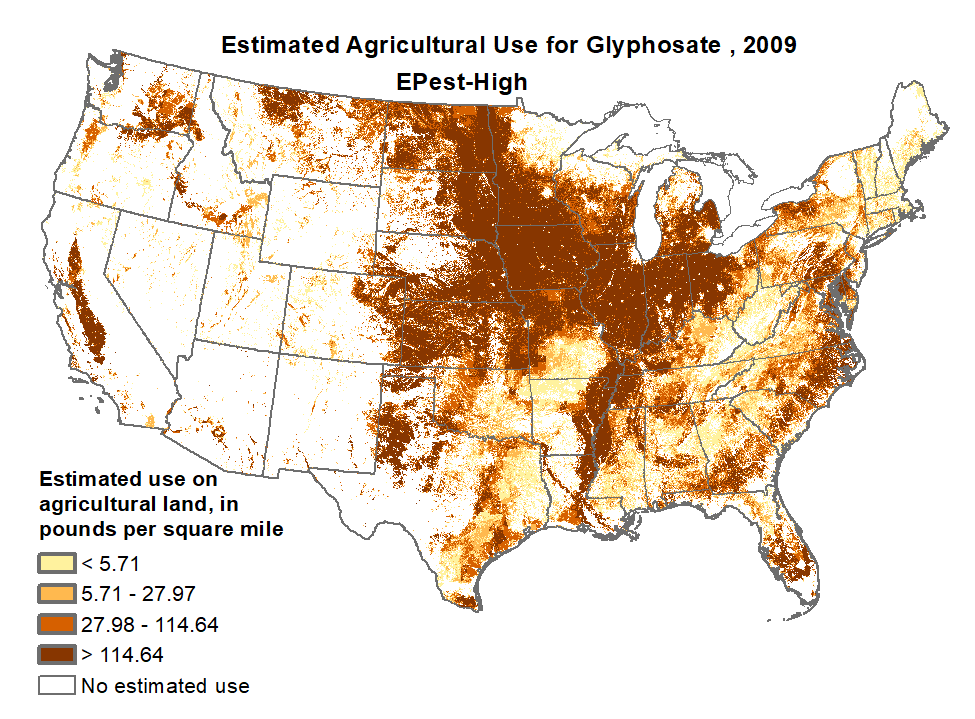
[INTERLUDE D – GLYPHOSATE (AKA THE ACTIVE INGREDIENT IN ROUNDUP)]
[INTERLUDE E – BAD SEEDS]
We come up with theories to try to make sense of the world around us, and we start by trying to come up with a theory that can explain as much of the available evidence as possible.
But one of the known problems with coming up with theories is that sometimes you are overenthusiastic, and connect together lots of things that aren’t actually related. It can be very tempting to cherry-pick evidence to support an idea, and leave out evidence that doesn’t fit the picture. It’s possible to make this mistake honestly — you get excited that things seem to fit together and don’t even notice all the evidence that is stacked against your theory.
But sometimes noticing that things seem to fit together is how an important insight comes to light. The theory of continental drift was invented when Alfred Wegener was looking through a friend’s new atlas and noticed that South America and Africa seemed to have matching coastlines, “like a couple spooning in bed”. He wasn’t even a geologist — at the time, he was an untenured lecturer in meteorology — but he thought that it was important, so he followed up on the idea. “Why should we hesitate to toss the old views overboard?” he said when his father-in-law suggested that he be cautious in his theorizing. He was criticized by geologists in Germany, Britain, and America, in part because he couldn’t describe a mechanism with the power to shuffle the continents around the globe. But in the end, Wegener was right.
The true power of a theory is its ability to make testable predictions. One obvious prediction of the theory that obesity is caused by a contaminant in our environment is that we should also expect to see paradoxical reactions to that contaminant.
Predicting Paradoxical Reactions
Sometimes drugs have what’s called a paradoxical reaction, where the drug does the opposite of the thing it normally does. For example, amphetamines are usually a stimulant, but in a small percent of cases, they make people drowsy instead. Antidepressants usually make people less suicidal, but sometimes they make people more suicidal.
Normally when we talk about paradoxical reactions, we’re talking about the intended effect of the drug, not the side effects. But from the drug’s point of view, there’s no such thing as side effects — all effects are just effects. As a result, we should expect to sometimes see paradoxical reactions in side effects as well.
And in fact, we do. A common side effect of the sedative alprazolam is rapid weight gain. But another common side effect is rapid weight loss. Clinical trials show both side effects regularly. One trial of 1,388 people found that 27% of patients experienced weight gain and 23% of patients experienced weight loss. In those who do lose weight, weight loss is correlated with the dose (r = .35, p = .006).
Severe weight gain is a common side effect of psychiatric drug clozapine. People can and do regularly gain ten or twenty pounds on this drug. But some people actually lose weight on clozapine instead.
Lithium increases leptin levels in most patients, and this is presumably part of the mechanism that causes people to gain weight on lithium. But in some patients, lithium reduces leptin levels instead.
Normally the weight loss from these paradoxical reactions is pretty limited. But occasionally people lose huge amounts. People can gain 4 lbs (1.8 kg) over only 17 days on alprazolam. In comparison, anecdotal reports from admitted abusers suggest that high doses of alprazolam can lead you to eventually lose 10 or even 40 lbs.
On clozapine, people usually gain 10-15 lbs. But some people lose huge amounts of weight instead, up to 50% (!!!) of their body weight. One patient, a woman in her 30s, went from about 148 lbs (67 kg) to about 75 lbs (34 kg) on clozapine.
AGRP neurons are a population of neurons closely related to feeding. One of the ways researchers established this connection was by showing that activating these neurons in mice led to “voracious feeding within minutes.” Another way they showed this connection was by destroying these neurons, a process called ablation. “AGRP neuron ablation in adult mice,” reviews one paper, “leads to anorexia.”
If weight gain is the main effect of a drug, the paradoxical reaction is weight loss. If the obesity epidemic is caused by one or more contaminants that cause weight gain, we should expect that there will be some level of paradoxical reaction as well. If obesity is the condition, the paradoxical condition would be anorexia.
If it’s possible to turn the lipostat up, leading to serious weight gain, it’s certainly possible to turn the lipostat down as well, leading to serious weight loss. For most people, these environmental contaminants cause weight gain. But just like with other drugs, in some people there’s a paradoxical reaction instead.
This is biologically plausible. People with anorexia have extremely low leptin levels, and some reports suggest that leptin levels are correlated with symptoms other than just BMI. Anorexia risk is genetically heritable and some of the genes involved have already been identified. The authors of one genetic analysis close by saying,
Low BMI has traditionally been viewed as a consequence of the psychological features of anorexia nervosa (that is, drive for thinness and body dissatisfaction). This perspective has failed to yield interventions that reliably lead to sustained weight gain and psychological recovery. Fundamental metabolic dysregulation may contribute to the exceptional difficulty that individuals with anorexia nervosa have in maintaining a healthy BMI (even after therapeutic renourishment). Our results encourage consideration of both metabolic and psychological drivers of anorexia nervosa when exploring new avenues for treating this frequently lethal illness.
Brain lesions alone can cause anorexia nervosa, complete with the characteristic psychopathologies like fear of fatness, drive for thinness, and body image disturbance. Many cases present as “typical” anorexia nervosa, complete with weight and shape preoccupations. When tumors are surgically removed, these symptoms go away and the patients return to a healthy weight.
Brain lesions are not the only purely biological issue that can cause anorexia. In some cases, it appears to be closely related to the gut microbiome. In one case study a patient with anorexia had a BMI of only 15 even after undergoing cognitive-behavioral therapy, medication, and short-term force feeding, and despite maintaining a diet of 2,500 calories per day. Physicians gave her a fecal microbiota transplant from an unrelated donor with a BMI of 25. Following the transplant she gained 6.3 kg (13.9 lbs) over the next 36 weeks, despite not increasing her calorie intake at all. This is only one case, but the authors indicate that they are planning to conduct a randomized controlled trial to investigate the effects of fecal transplants in individuals suffering with anorexia. To the best of our knowledge this next study has not yet been published, but we look forward to seeing the results.
Eating and maintaining weight is a central cognitive problem. “The lipostat does much more than simply regulate appetite,” says Stephan Guyenet, “It’s so deeply rooted in the brain that it has the ability to hijack a broad swath of brain functions, including emotions and cognition.”
Remember those children we mentioned in Part II, who were born without the ability to produce leptin? Unlike normal teenagers, they aren’t interested in dating, films, or music. All they want to talk about is food. “Everything they do, think about, talk about, has to do with food,” says one of the lead researchers in the field. A popular topic of conversation among these teens is recipes.
These teenagers have a serious genetic disorder. But if you put average people in a similar situation, they behave the same way. The Minnesota Starvation Experiment put conscientious objectors on a diet of 1,560 calories per day. Naturally, these volunteers became very hungry, and soon found themselves unable to socialize, think clearly, or open heavy doors.
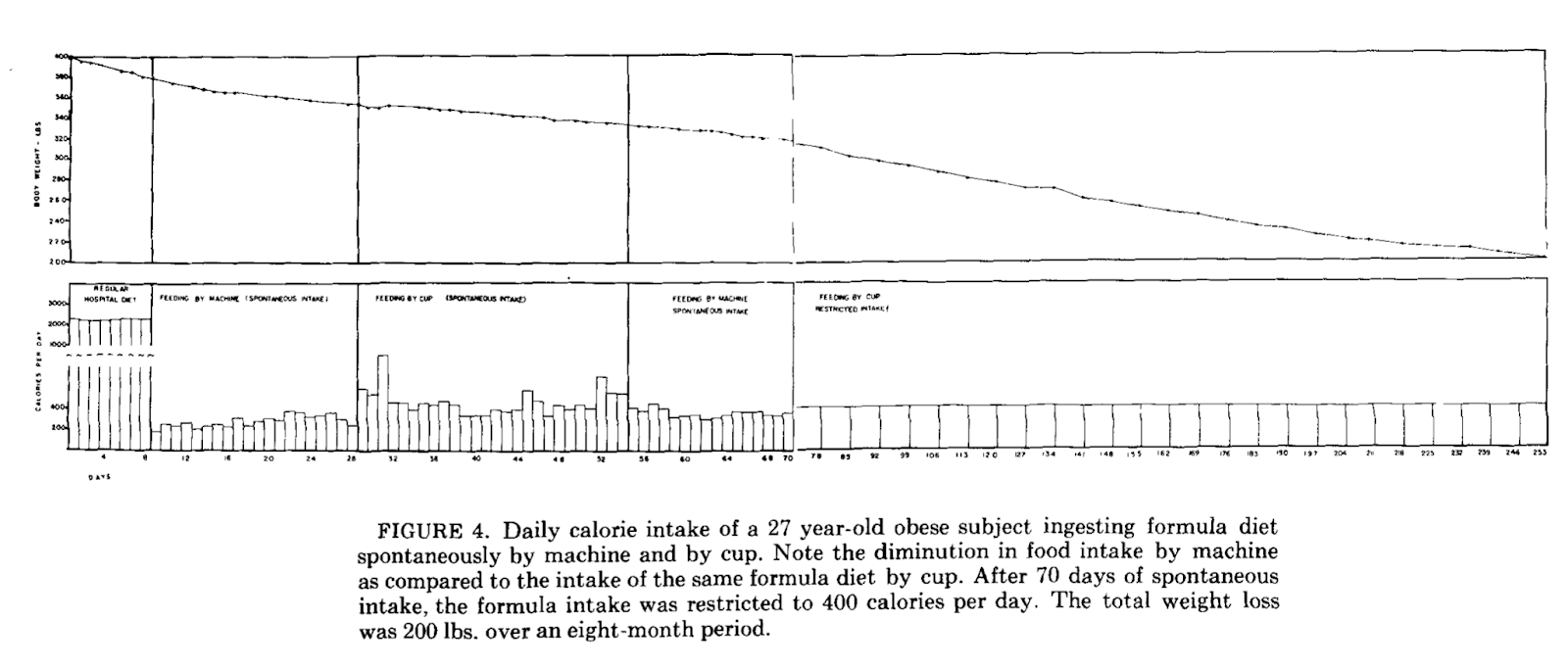
As they lost weight, these men developed a remarkable obsession with food. The researchers came to call this “semistarvation neurosis”. Volunteers’ thoughts, conversations, dreams, and fantasies all centered on food. They became fascinated by the paraphernalia of eating. “We not only cleaned our plates, we licked them,” recalled one volunteer. “Talked about food, thought about it. Some people collected as many as 25 or 30 cookbooks” (one such collection is pictured below). Others collected cooking utensils. “What we enjoyed doing was to see other people eat,” he continued. “We would go into a restaurant and order just a cup of coffee and sit and watch other people eat.”
These are the neuroses of people whose bodies believe that they are dangerously thin, either correctly (as in the starvation experiment) or incorrectly (as in the teenagers with leptin deficiency). The same thing happens when your mind, correctly or incorrectly, believes that you are dangerously fat. You become obsessed with food and eating, only in this case, you become obsessed with avoiding both. A classic symptom of anorexia is “preoccupations and rituals concerning food”. If that doesn’t describe the behavior above, I’m not sure what would.
But avoiding food and collecting cookbooks isn’t the lipostat’s only method for controlling body weight. It has a number of other tricks up its sleeve.
Many people burn off extra calories through a behavior called “non-exercise activity thermogenesis” (NEAT). This is basically a fancy term for fidgeting. When a person has consumed more calories than they need, their lipostat can boost calorie expenditure by making them fidget, make small movements, and change posture frequently. It’s largely involuntary, and most people aren’t aware that they’re burning off extra calories in this way. Even so, NEAT can burn off nearly 700 calories per day.
When most people eat less than they need, they become sluggish and fatigued, like the volunteers in the Minnesota Starvation Experiment. But people with anorexia fidget like crazy. A classic symptom of anorexia is excessive physical activity, even in the most severe stages of the illness. When one group measured fidgeting with a highly accurate shoe-based accelerometer, they found that anorexics fidget almost twice as much as healthy controls.
This kind of fidgeting is the classic response in people whose bodies are fatter than they want to be. In studies where people were overfed until they were 10% heavier than their baseline, NEAT increased dramatically. All of this is strong evidence that people with anorexia have lipostats that mistakenly think they desperately need to lose weight.
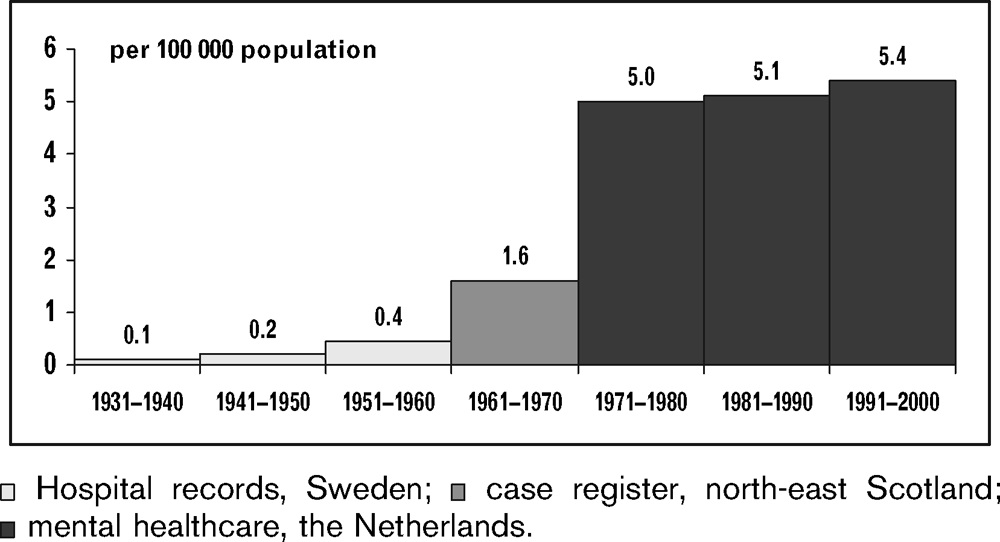
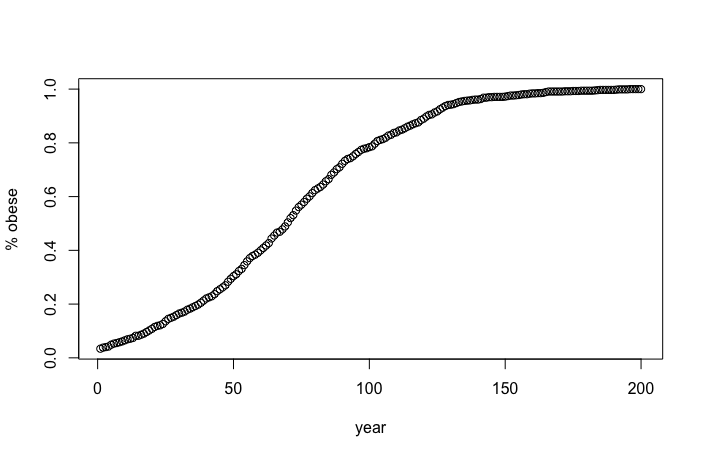
Of course, this does sound a little far-fetched. If anorexia were really a paradoxical reaction to the same contaminants that cause obesity, then in the past we would see almost no anorexia in the population, up to a sharp spike around 1980…
While there’s not as much historical data as we would like, the pattern we observe is just about that (see figure below). Cases were quite low until about 1970, when prevalence suddenly shot up. When we look at specific sections of historical data, finding evidence of an increasing trend (often only in young women) is pretty common.
In general the data is pretty scattered and spotty. Rarely does a study look at rates in the same area for more than five years. When there are such comparisons, they are usually for periods before 1980. For example, van’t Hof and Nicolson, writing in 1996 and arguing that rates of anorexia are not increasing, at one point cite studies that showed no increase from 1935-1979, 1935-1940, 1975-1980, and 1955-1960. But data from the Global Health Data Exchange (GHDx) shows that rates of eating disorders have been increasing worldwide since 1990, from about 0.185% to 0.215%. This trend is small but reliable — 87.5% of countries saw their rates of eating disorders increase since 1990.
(If that’s not enough for you, we can mention that in 1985 the New York Times reported, “before the 1970’s, most people had never heard of anorexia nervosa.” Writing in the 1980s, presumably they would know.)
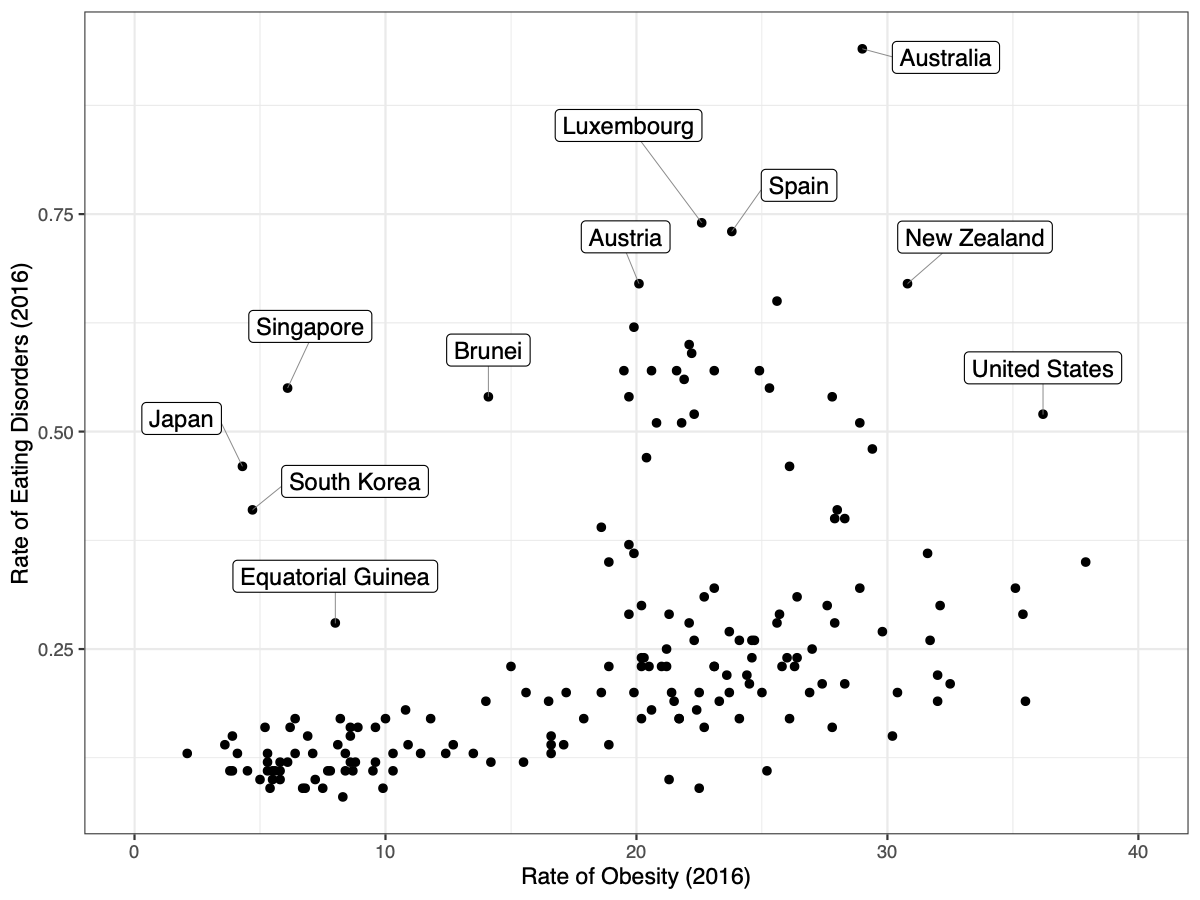
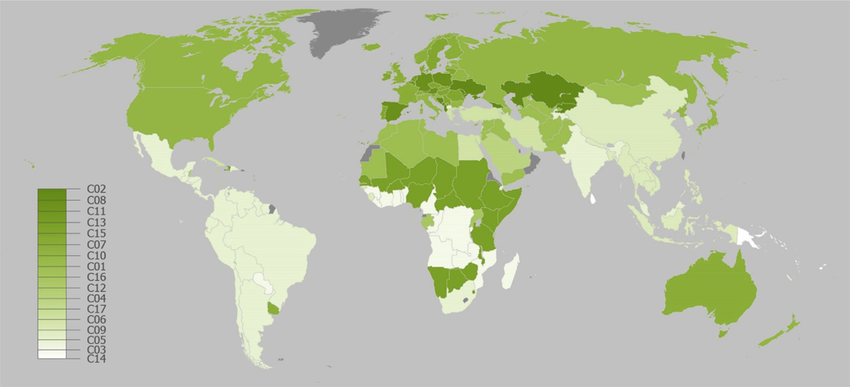
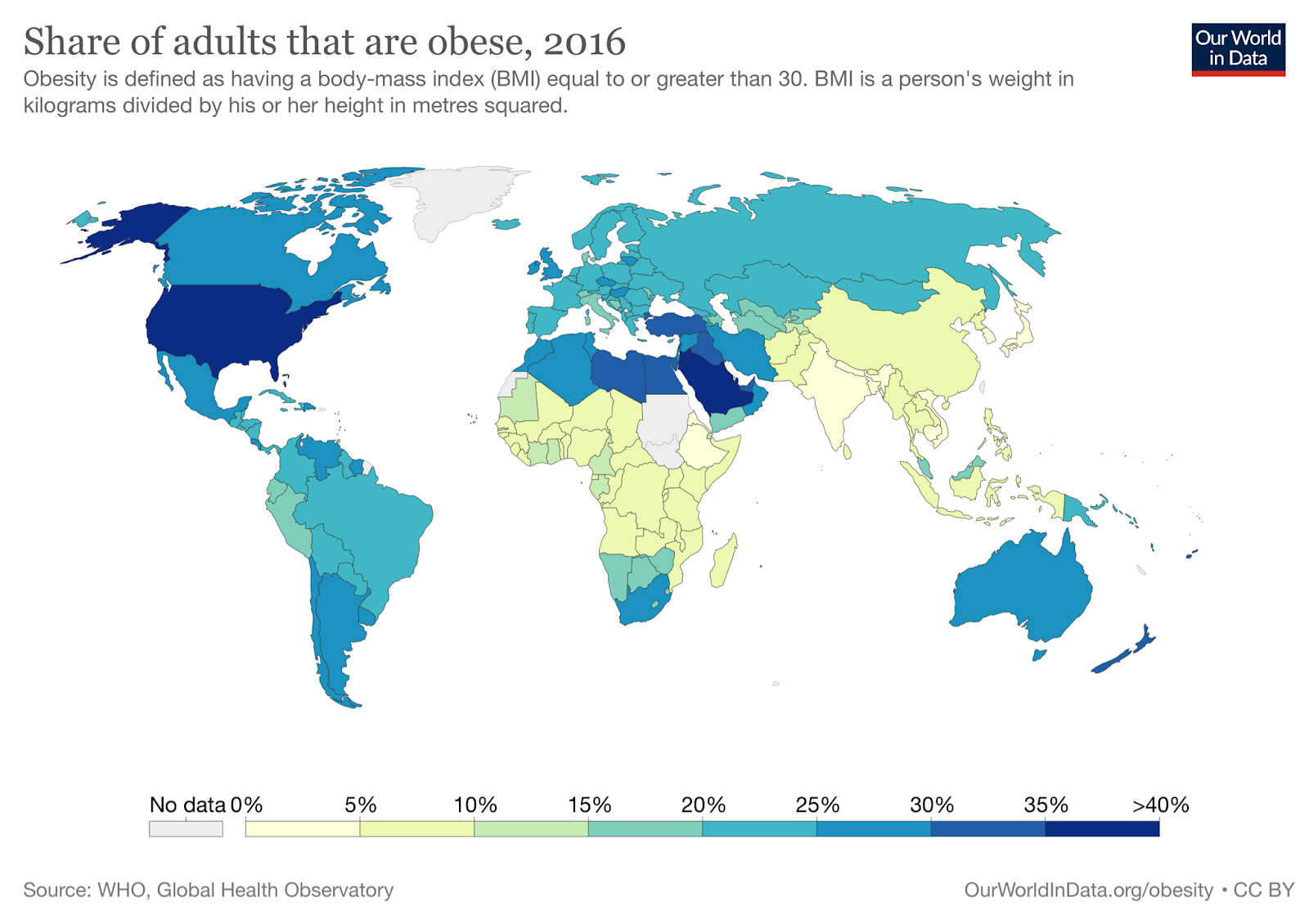
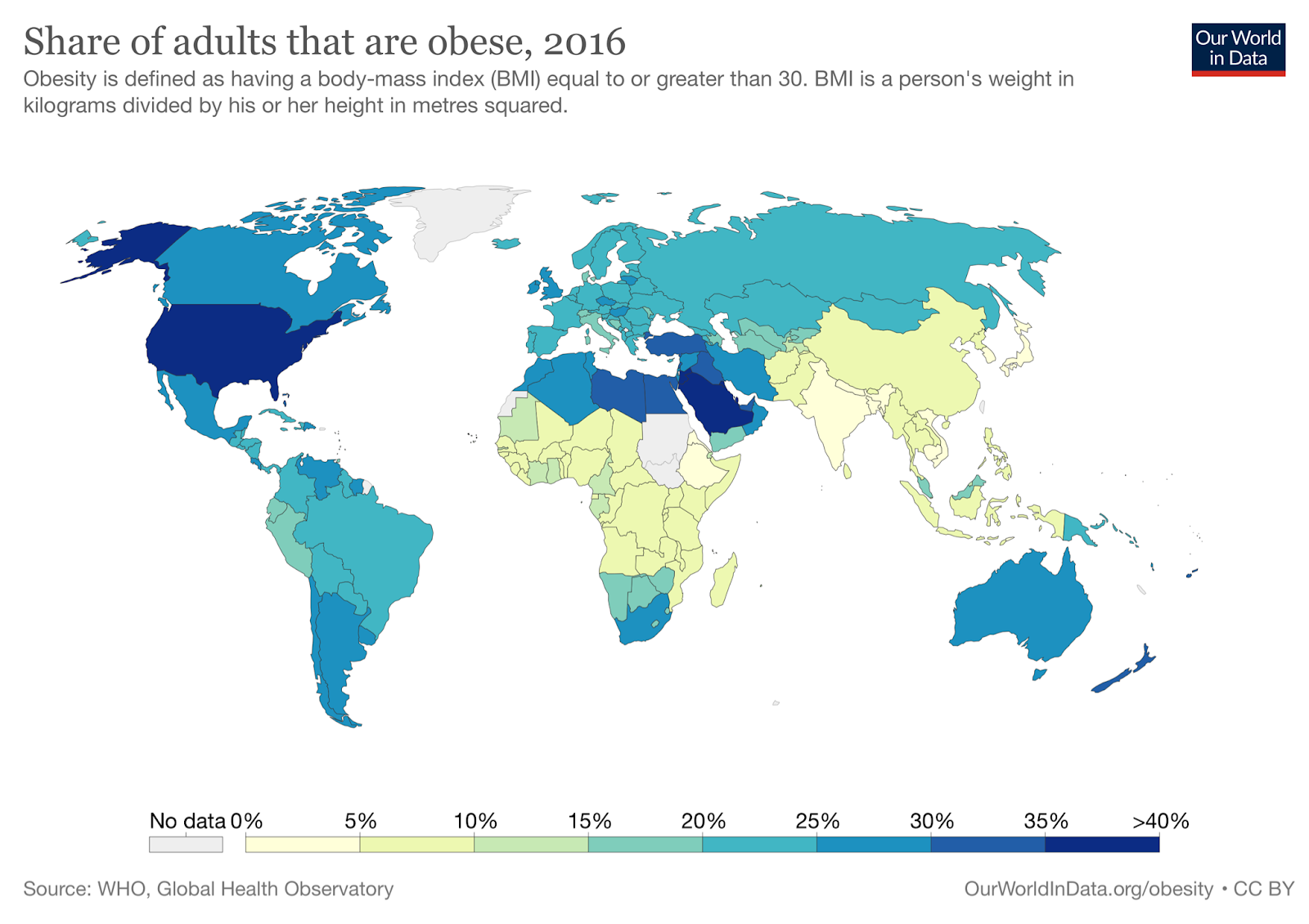
There are other ways to look at the relationship. For example, we can compare the most obese countries to the countries with the highest rates of eating disorders:
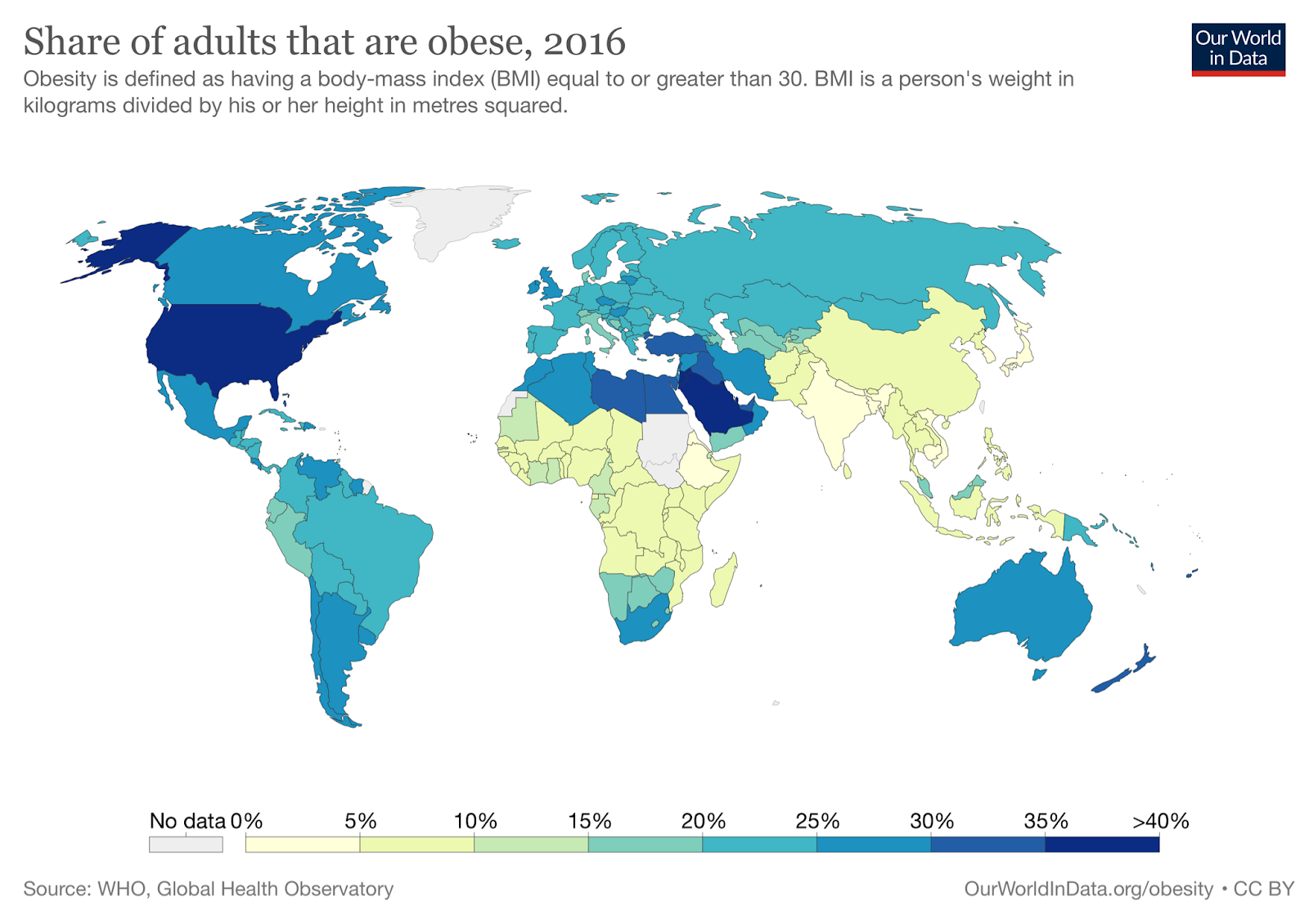
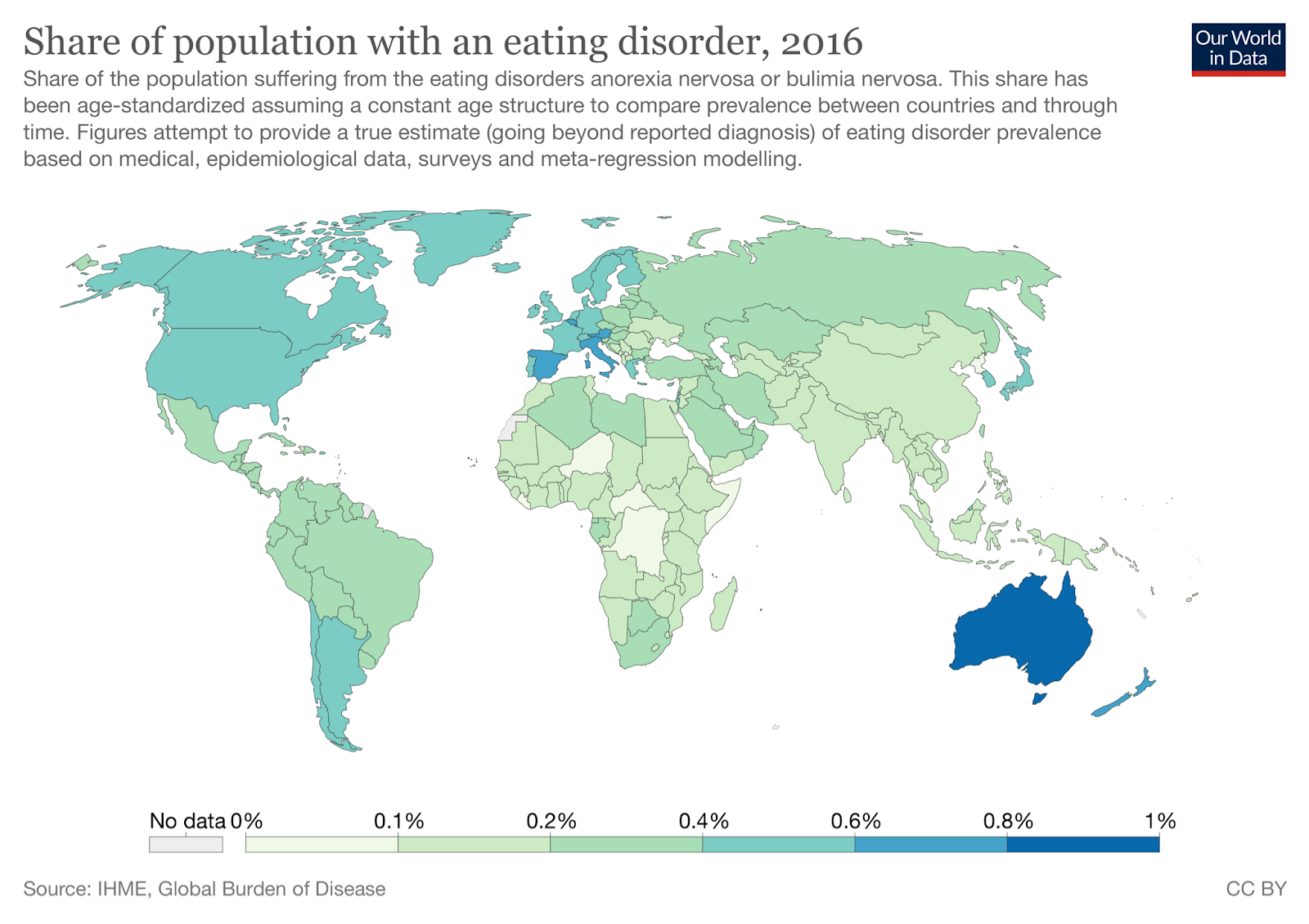
With the exception of a few notable outliers (genetically homogeneous South Korea and Japan), these match up really well. The fit isn’t perfect, but we shouldn’t expect it to be. There are large genetic differences and differences in healthcare practices between these countries. They may use different criteria to diagnose eating disorders. But even given these concerns, we still see pretty strong associations — Chile, Argentina, and Uruguay are the most obese countries in South America, and they also have the highest rates of eating disorders.
We can go one step further. Looking at the data, we see that these are statistically related. In 2016, rates of eating disorders were correlated with obesity in the 185 countries where we have measures for both, r = .33, p < .001. If we remove the five tiny island nations with abnormally high (> 45%) obesity (Kiribati, Marshall Islands, Micronesia, Samoa, and Tonga), all of them with populations of less than 200,000 people, the correlation is r = .46:
We see the same correlation between rates of obesity and rates of eating disorders when we look at the data from 1990, r = .37, p < .001.
Perhaps most compelling, we find that the rate of change in obesity between 1990 and 2016 is correlated with the rate of change in eating disorders between 1990 and 2016. The correlation is r = .26, p = .0004, and it’s r = .30 if we kick out Equatorial Guinea, a country where the rates of eating disorders tripled between 1990 and 2016, when none of the other countries even had their rates double. You can see those data (minus Equatorial Guinea) below:
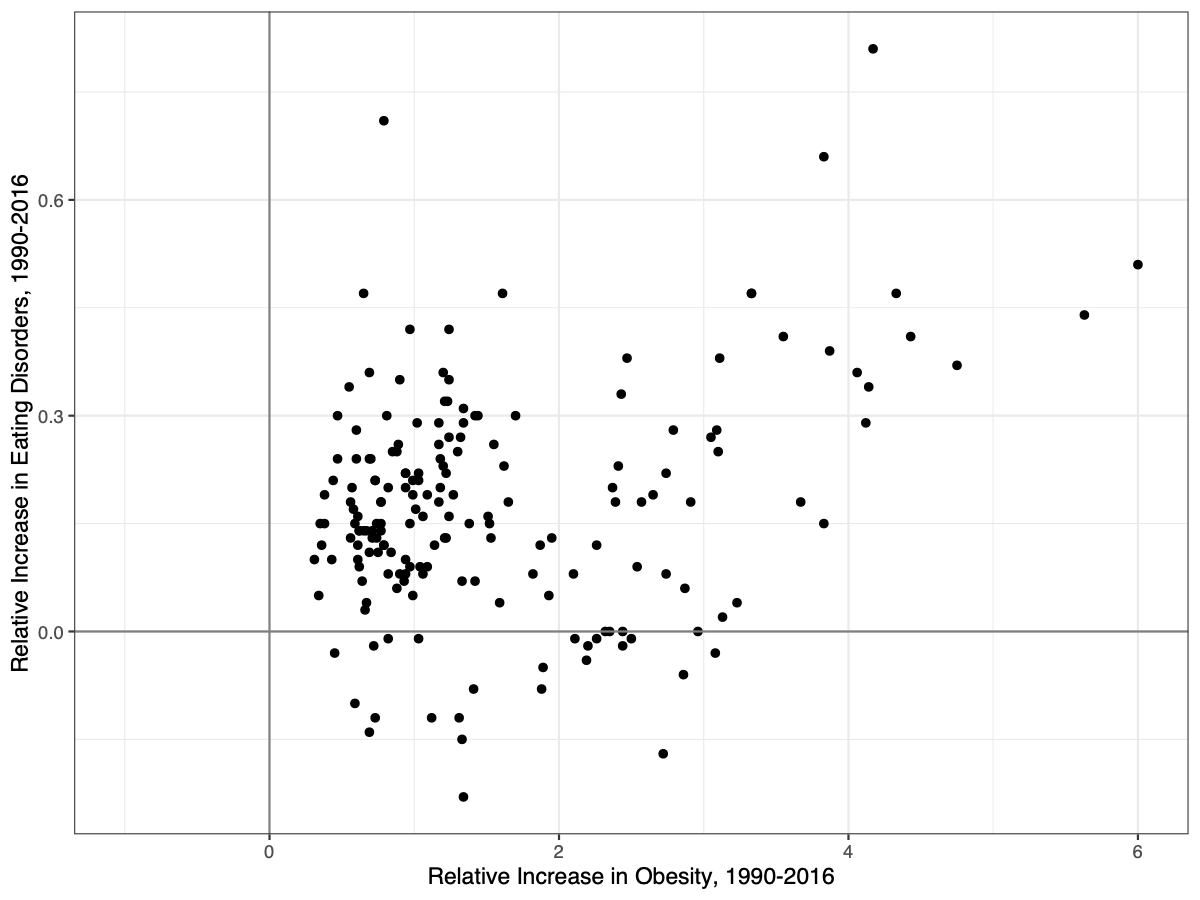
That’s no joke. The countries that are becoming more obese are also having higher and higher rates of eating disorders.
We even see signs of a paradoxical reaction in some of the contaminants we reviewed earlier. You’ll remember that when mice are exposed to low doses of PFOA in-utero, they are fatter as adults — but when mice are exposed to high doses as adults, they lose weight instead. The dose and the stage of development at exposure seems to matter, at least in mice. It’s notable that anorexia most often occurs in teenagers and young adults, especially young women. Are young women being exposed to large doses all of a sudden, just as they start going through puberty? Where would these huge doses come from? It may not be that much of a stretch — PFAS are included in many cosmetics.
In one study of 3M employees, higher PFOS levels led to a higher average BMI, but also to a wider range in general. The lightest people in the study had some of the highest levels of PFOS in their blood. The quartile with the least PFOS in their blood had an average BMI of 25.8 and a range of BMIs from 19.2 to 40. The quartile with the most PFOS in their blood had an average BMI of 27.2 and a range of BMIs from 17.8 to 45.5. Remember, a BMI of below 18.5 is considered underweight.
In the study of newborn deliveries in Baltimore that we mentioned earlier, researchers found that obese mothers had babies with higher levels of PFOS than mothers of a healthy weight. But underweight mothers also had babies with higher levels of PFOS. In fact, babies from underweight mothers had the highest levels of PFOS exposure, 5.9 ng/mL, compared to 5.4 ng/mL in obese mothers, and 4.8 ng/mL in mothers of normal weight. “The finding that levels were higher among obese and underweight mothers is interesting,” they say, “but does not have an obvious explanation.” Knowing what we know now, the obvious explanation is that PFOS usually causes weight gain, but like all drugs, it sometimes has a paradoxical reaction, resulting in weight loss instead.










{kind=link}