When it comes to chronic illnesses, most people try to find ways to avoid the pain. This is because pain bad, and no pain, good.
But we worry that avoiding pain is good in the short term but bad in the long term; penny wise and pound foolish.
If you’re worried that pizza makes you bloated, it’s good common sense to try to avoid pizza. But it’s bad science. Past a certain point, avoiding pizza tells you nothing. To learn something more, you have to bite the bullet.
Better to wait for a day when you feel great, no bloating at all, and then intentionally go and eat pizza, and see what happens. Or each afternoon you feel good, flip a coin, and eat pizza when it comes up heads. Do this a couple of times. If you do this, you should be able to see if pizza is really a reliable trigger for your bloating.
There are two reasons to do this. The first is — what is it about pizza that makes you bloated? If you can show that pizza is a trigger, you can start doing empirical splits. Buy the same pizza and flip a coin. If it’s heads, scrape off the cheese and tomato and just eat the bread. If it’s tails, toss the bread and just eat the cheese and tomato scraped off into a bowl. Which makes you bloated? If it’s the cheese and tomato, separate them and do the same thing.
So we did this half-tato diet community trial. People signed up for a minimum of six weeks — two weeks of baseline, so we could see how their weight changed when they were eating as normal, and then four weeks where they got around 50% of their calories from potatoes every day.
This was inspired by our original Potato Diet Community Trial, which worked pretty well. In that study, people lost an average of 10.6 lbs over four weeks eating almost nothing but potatoes.
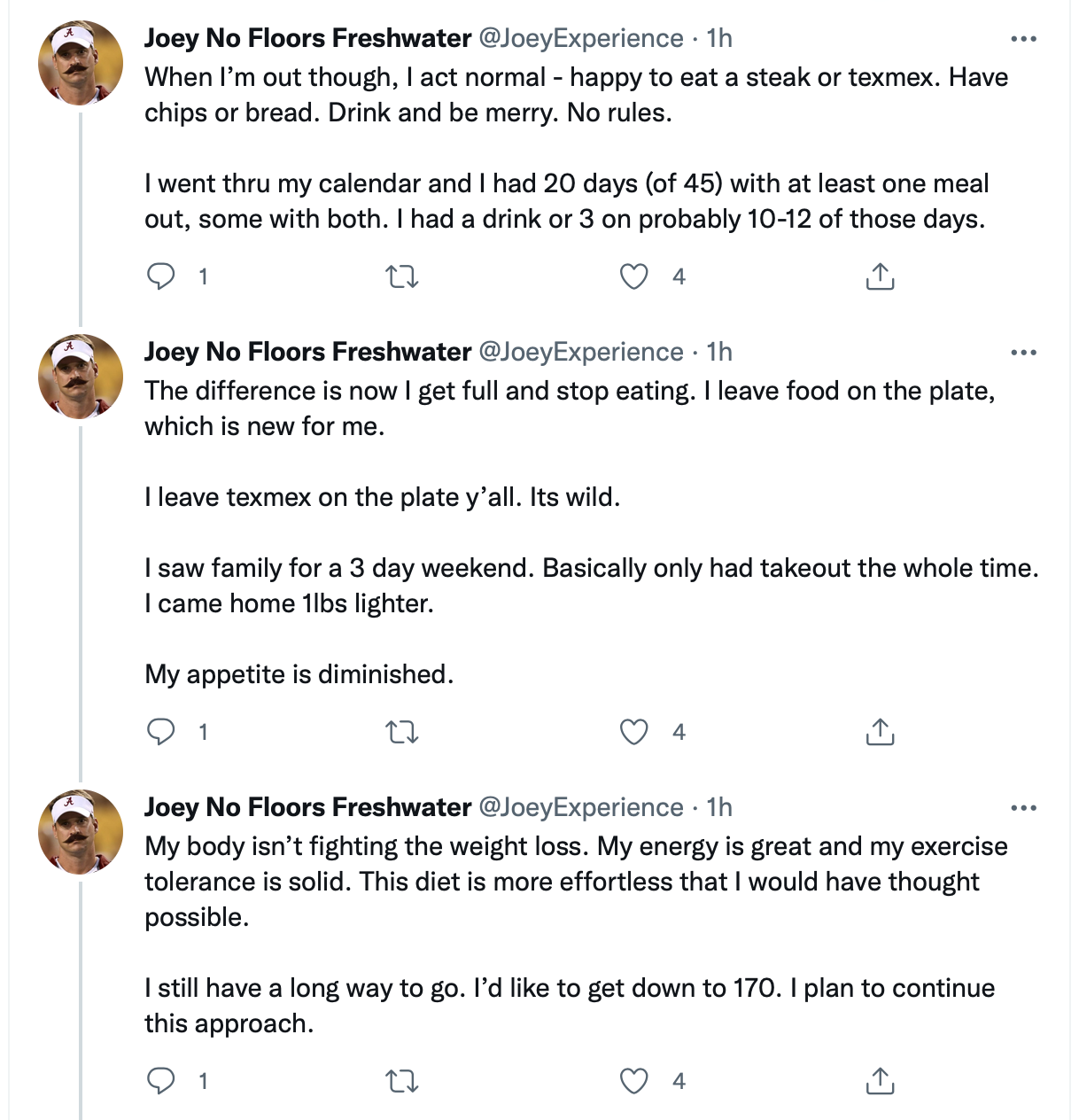
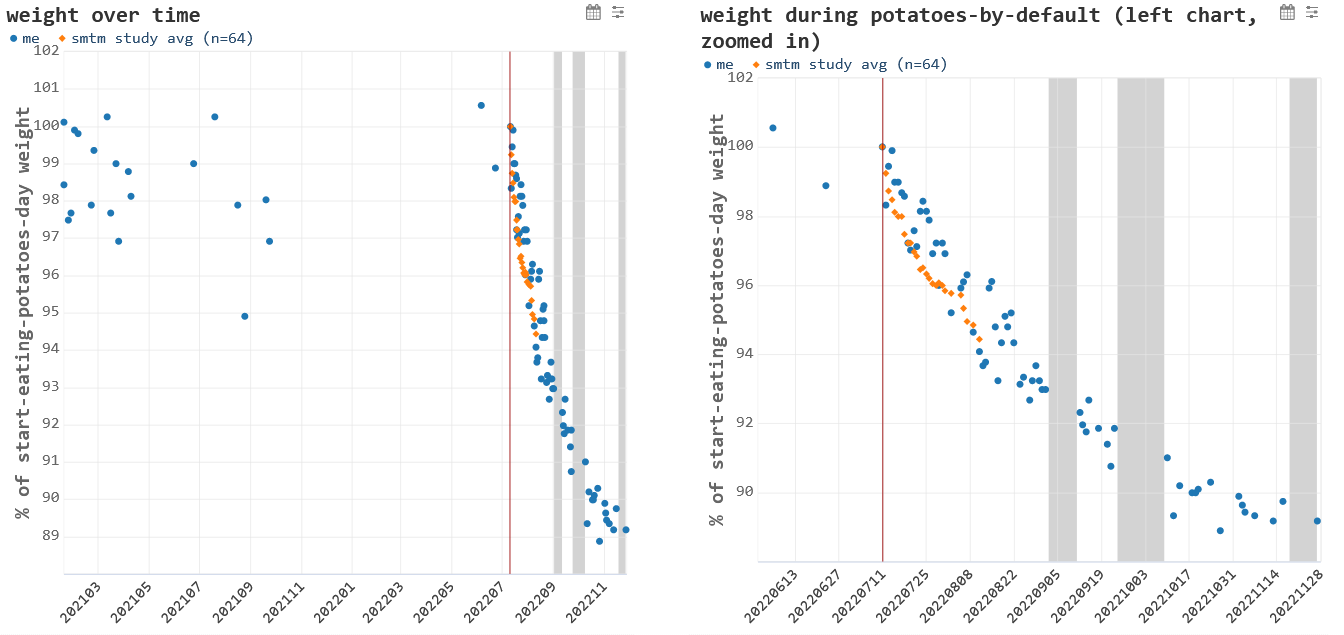
We say “almost nothing but potatoes” because most people took multiple cheat days, and it didn’t seem to make much of a difference. Combined with a couple of case studies, who reported enormous success on a half-tato diet (in particular, M with his potatoes-by-default), this made us wonder if a half-tato diet could be made to work almost as well as a full-tato diet.
Anyways, let’s look at some results.
Today’s analysis is based on a snapshot of the data taken on June 1, 2023 (about 10 weeks after the study was launched). This means we have up to 10 weeks of data, specifically 2 weeks of baseline and 8 weeks of half-tato. A few people are still going with the half-tato diet, but we will look at their data later.
The dataset is mostly straightforward, but here’s one note: One or two important measurements were missing for a small number of people. For example, they might have entered a weight for Day 28 and Day 30, but not Day 29 (which is important because Day 29 is the end of the first four weeks).
When an important measurement like this was found to be missing, we filled it in by making the missing measurement the average of the two values around it. For example, if the weight measurement for Day 29 was missing, we filled it in with the average of the weights on Day 28 and Day 30.
We did all these replacements before doing the analysis, and only a few measurements were interpolated like this.
As usual: raw data, the analysis script, and study materials are available on the OSF.
Participants
A total of 123 people filled out the signup form.
Of those, 8 people filled out the form incorrectly in such a way that we couldn’t sign them up (they didn’t enter an email, didn’t enter critical data such as height, etc.). We enrolled the remaining 115 people in the study.
Of the 115 people who were enrolled, 92 entered at least one day of weight data.
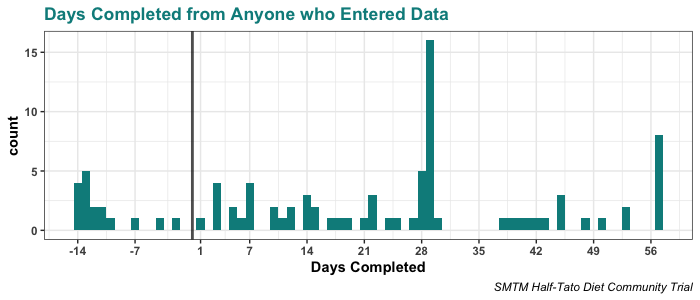
For people who entered any data, the most common outcome was to make it the full 2 weeks baseline + 4 weeks half-tato, though people dropped out at various points along the way, and a few people didn’t finish the baseline two weeks.
Here you can see how many days people completed. In this figure, the vertical line at 0 divides the baseline span (Days -14 to -1) from the half-tato span of up to 8 weeks (Days 1 to 57).
Let’s summarize that plot. As of the snapshot on June 1st:
92 people entered at least one day of weight data
75 people made it to Day 1, past the baseline period of two weeks
38 people made it to Day 29, the end of the first 4 weeks of half-tato
8 people made it to 8 weeks or further, and some are still going
For this analysis, we will mostly be focusing on weight change up to Day 29, since there’s not much data past that point.
Weight Change over Baseline
First let’s look at the baseline. Similar to a crossover design, this baseline serves as a kind of control group.
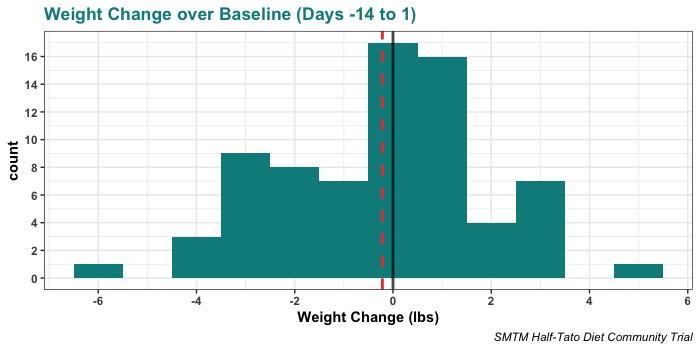
There was very little average weight change in the baseline period, and it was not statistically distinguishable from zero. Here’s the histogram of weight change over baseline, with a black vertical line at 0 lbs (i.e. no weight change over baseline) and a red dashed vertical line at the mean weight change:
The mean weight change over this period was -0.22 lbs, with a 95% CI of -0.70 lbs to 0.27 lbs. This is not statistically distinct from zero.
The mean suggests an average loss of 0.11 lbs per week on average, or 0.35 per week if we take the lower bound of the confidence interval.
Of course, it’s also consistent with an average weight GAIN of 0.14 lbs per week if we take the upper bound of the confidence interval.
In previous studies, people have expressed concern about the Hawthorne effect— that when we ask people to measure their weight, they might start losing weight simply because they are aware that their weight is being observed. Looking at the baseline period, we find very little support for this idea, even with a sample size of 75 people.
Observing your weight for two weeks just doesn’t change it much, and likely doesn’t change it at all. Going forward, we will continue to not worry about the so-called Hawthorne effect.
(Also, it’s amusing to see that Wikipedia kind of drags this whole idea: “some scholars feel the descriptions are fictitious” and “J. G. Adair warned of gross factual inaccuracy in most secondary publications on the Hawthorne effect and that many studies failed to find it.”)
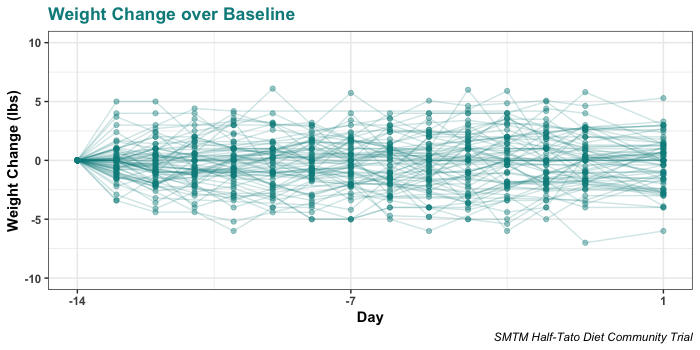
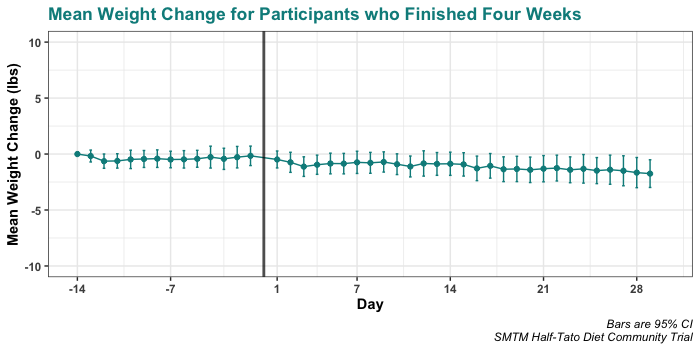
Here’s a plot of weight change over baseline, including only people who finished the two-week span. As you can see, these look like a bunch of random walks around zero.
Weight Change at Four Weeks
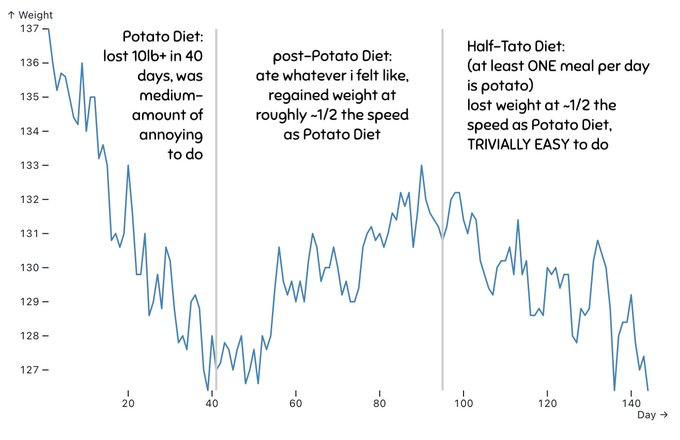
Our main interest is weight change on the half-tato diet, specifically people’s weight change between the morning of Day 1 and the morning of Day 29. Here’s the histogram of that variable, with a black vertical line at 0 lbs (i.e. no weight change over 29 days) and a red dashed vertical line at the mean weight change:
People lost 1.7 lbs on average over these four weeks, and that loss is significantly different from zero, t(37) = 2.70, p = .010. Another way of putting this is that 27 out of 38 people (71%) lost at least some weight.
By now we’re sure you’ve noticed the extreme outlier, the person who reported losing 17 lbs over four weeks (participant 25348806). This outlier is impressive, and we’ll look at her results in more detail later, but excluding that person doesn’t change the overall results. Without the outlier, average weight loss is 1.3 lbs over four weeks, and that loss remains significantly different from zero, t(36) = 2.66, p = .012.
We see that weight loss is significantly different from zero. People do seem to lose weight on the half-tato diet.
But we should also emphasize that they don’t lose much — the effect size here is a disappointment. We had hoped that the half-tato diet might have around half the effect of the full potato diet, but that just didn’t happen.
Overall, the effect is less than half the effect of the original potato diet. Average weight loss on the potato diet was 10.6 lbs, so half of that would be 5.3 lbs. Instead we see only around 15% of the effect of the full-tato diet.
We should note that there are some mitigating factors here. In particular, about 30% of participants in the half-tato diet started out as “normal weight” (BMI < 25), compared to only about 15% in the original potato diet. (In the original study, people who were obese or overweight tended to lose more weight, so this means the average weight loss will look smaller when there are fewer obese or overweight participants.)
But weight loss on half-tato is still quite minor, even if you limit the analysis just to overweight (BMI > 25) participants, who lost 1.8 lbs on average, or obese (BMI > 30) participants, who lost 3.1 lbs on average. This is still much less weight loss than on the original potato diet.
Another way to put it is like so: On the original potato diet, 64 people made it 4 weeks. One of those people lost no weight. Everyone else lost more than the AVERAGE weight loss on the half-tato diet. It’s really no contest; full-tato is overwhelmingly more reliable and causes overwhelmingly more weight loss, at least among the people who can make it four weeks on mostly potatoes.
Frankly, this just emphasizes how successful the original potato diet study was. In fact, on reflection the Potato Diet Community Trial was probably the most successful weight loss study of all time. Are there any other studies that caused weight loss in 98% of people who finished the study, and caused an average of 10.6 lbs of weight loss over just four weeks? Not that we know of.
Trajectory
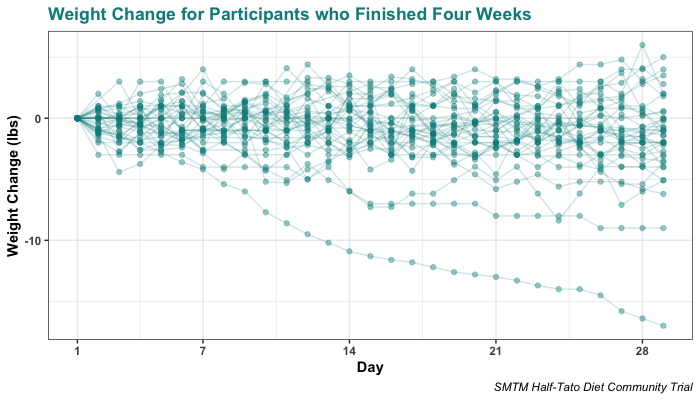
As we mentioned, there’s one extreme outlier who lost 17 lbs over four weeks. You may also have noticed a less-extreme outlier who lost 9 lbs, who happens to be someone who participated in the original Potato Diet Community Trial and saw a lot of weight loss there as well, losing 19 lbs. Both of them stand out quite clearly in a plot of people’s weight loss trajectories:
Having seen some reports like this one, we wondered if there might be a yo-yo effect on the half-tato diet, where in the beginning people lose weight no problem, but at some point the potato effect stops working and their weight heads back to baseline. That seems like a reasonable way to interpret this plot:
But overall, this doesn’t seem to be the case. In general, half-tato weight loss over four weeks seems small but constant:
Weight Change at Eight Weeks
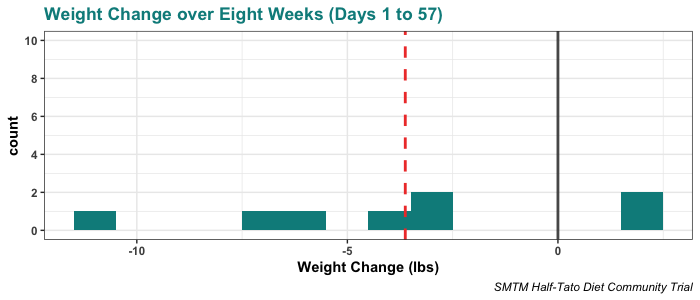
We also have a tiny bit of data on people’s weight loss taking the half-tato diet out to eight weeks. Here’s the plot:
The average weight loss at eight weeks is 3.6 lbs, though you can see that one person has lost more than 10 lbs. With only eight individuals, this is too few people to do a statistical analysis. But it does suggest that longer spans on the half-tato diet may be effective.
Note that the extreme outlier does not appear in this group — that person only sent us data up to Day 29.
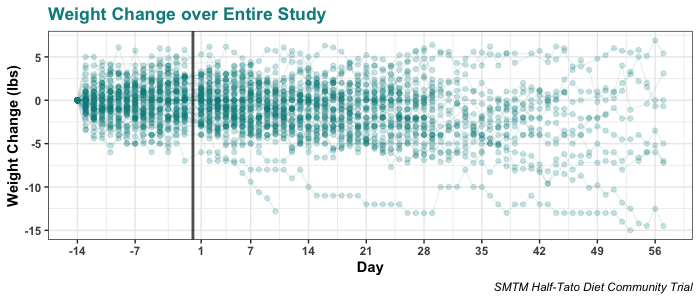
Here’s the whole span from everyone who finished baseline (minus our main outlier), showing all data points from the start of baseline to the end of eight weeks:
What Things Correlate with Weight Loss
There’s not much variation in people’s weight loss over these four weeks, but some people did lose more weight than others. This makes us wonder if there are any variables that might be correlated with weight loss.
Take the analyses below with a grain of salt. They’re very exploratory. The sample size is small. We’re not correcting for multiple comparisons. And of course, all these correlations are correlational.
As you well know, correlation does not imply causation — but as XKCD reminds us, “it does waggle its eyebrows suggestively and gesture furtively while mouthing ‘look over there’.” Correlations can still be suggestive, and if any of the correlations we find are real, we should eventually be able to demonstrate the same relationships experimentally. So let’s take a look and see if anything stands out.
BMI
Our first surprise is that BMI doesn’t seem to have much to do with weight loss.
The correlation between weight loss and starting BMI is relatively small, and is not statistically significant, r(36) = -0.29, p = .078.
Protocol
We let people sign up for three different protocols for the half-tato diet, three different ways you could try to get about 50% of your calories from potatoes. People ended up about evenly split between the three approaches:
Here is a plot of weight loss by each of the protocols:
As you can see, there are no huge differences in weight loss between the three protocols, though Potatoes-By-Default includes the outlier who lost the most weight.
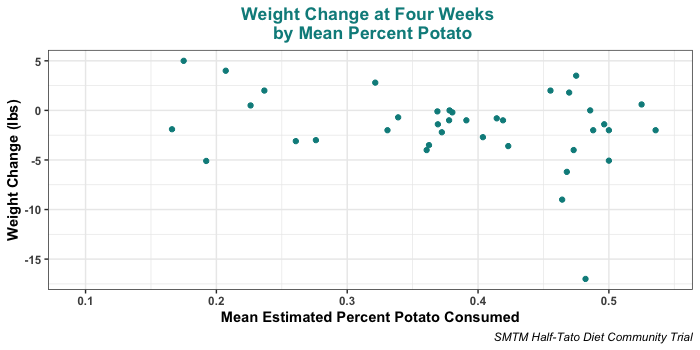
Percent Potato
We asked people to estimate what percent of their total calories they were getting from potatoes each day, and some people reported getting a much higher percent potato than others. Since some people were doing about 50% potato, and others were doing only about 10%, you might suspect that the diet caused more weight loss for people getting more potato.
This is much more muddy than we expected. Getting closer to 50% of your calories from potatoes does seem to maybe cause more weight loss, but if so, it’s not super clear. The correlation is quite small and not significant, r(36) = -0.28, p = .084, and weaker if you exclude the major outlier, r(35) = -0.24, p = 0.147.
It’s hard to imagine that percent potato doesn’t matter at all, and we do see that the three people who lost the most weight were all getting close to 50% potato. This suggests that for best results, you should try to get around 50% potato on average. But there isn’t a clear correlation overall.
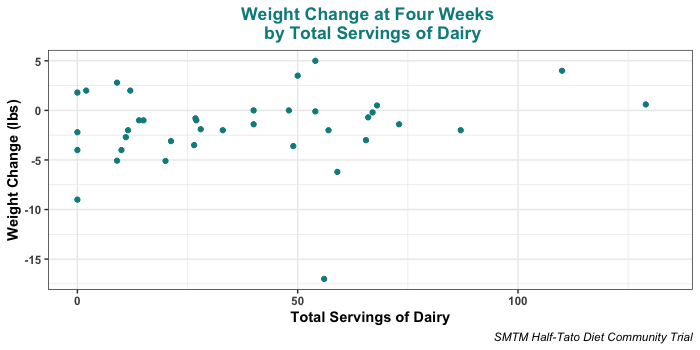
Dairy
In the original Potato Diet Community Trial, we asked people to avoid dairy entirely. This time around, we decided to just ask people to track how many servings of dairy they got each day. This lets us look for any correlation between dairy consumption and weight loss on half-tato.
There may be a bit of a trend where more dairy is related to less weight loss, but the person who lost the most weight ate plenty of dairy, and the overall correlation is not significant, r(36) = 0.15, p = .355.
That said, the relationship is slightly stronger if we exclude the outlier, though still not significant, r(35) = 0.29, p = .078.
Tomato
We were also concerned that tomato products might interfere with potato-based weight loss. So just like dairy, we asked people to track how many servings of tomato products they had each day. Here’s the scatterplot:
Surprisingly, this relationship is significant, even with such a small sample. The overall correlation is r(36) = 0.37, p = .021, and it remains significant if you remove the extreme outlier, r(35) = 0.36, p = .031.
You can see that the two outliers, people who lost the most weight, almost entirely avoided tomato products on the diet. Also interesting is that the person who gained the most on the diet happens to be the person who ate the most servings of tomato products.
This is correlational, not corrected for multiple comparisons, etc., but it does provide more support for our suspicion that tomatoes interfere with the potato weight loss effect. This would be great to experimentally confirm at some point, and it should be relatively easy to test — just assign some people on a potato diet to use ketchup, and others to eat their potatoes bareback, i.e. no ketchup. In the meantime if you are trying to lose weight using potatoes, we certainly encourage you to avoid ketchup.
Cooking Method
We’ve previously mentioned that boiling or soaking potatoes removes a lot of their potassium. So we’re curious to see if people who boiled their potatoes lost less weight than people who baked, roasted, fried, or otherwise kept their potatoes for the most part whole and un-leached.
Most people didn’t leave detailed notes on how they prepared their taters, but the people who did leave notes often mentioned either boiling them or using frozen potato products, which are generally pre-boiled / blanched / parboiled.
This might explain why the half-tato diet did not cause much weight loss on average — if we’re right, and the weight loss is caused by potassium (or anything else in the potatoes that is leached out on boiling/blanching/soaking; who knows, maybe iodine), then many people were consuming less effective potatoes.
There aren’t enough reports to bother hand-coding preparation method or doing an analysis, but here are some examples:
(42475044) Most of my potato meals were a 50/50 mix of roasted yellow potatoes (partially peel 1 inch cubes, lightly oil, 375 convection for 45 minutes), and store-bought frozen french fries (whatever seemed to have the least oil) cooked in the air fryer with no additional oil.
(63062664) My protocol was mostly whole boiled potatoes pan-fried in ~15g of butter or a small glug of rapeseed or olive oil. Usually ~1kg for breakfast + lunch.
(78152385) I ate mainly russet or golden potatoes, baked or roasted, and I didn’t eat the skins of the russet because last time I did that it gave me the worst stomach cramps I’ve ever had. I also ate a lot of Alexia french fries with sea salt, and some sweet potatoes.
(80975703) I always ate potatoes I had boiled in batches and kept in the fridge. My favourites were red potatoes, half peeled, but I also had yellow or white potatoes, fully peeled. Always with a bit of olive oil and salt and spices, chopped up and reheated in a pan on the stove.
(28228309) I had visions of making home-made latkes or really fine hash browns. I just didn’t make time. While I know we are supposed to start with whole potatoes, I’m sure glad I found frozen potato patties at the store, or there’s no way I could’ve even approximated the quantity of potato I needed. I put my toaster to 6 (nearly the highest setting) and toast them twice, and they’re great, and I could do it for breakfast on work days.
(30834698) I do not like skin on the potatoes; I can eat it, but I do not like the taste or how it makes me feel; I prefer them without skin, so I mostly eat them like that; usually just boiled with a pinch of salt, sometimes in the oven, sometimes with a drop of olive oil; sometimes with some harissa; the easiest and tastiest for me was boiled with salt, then peel the skin and eat them
(72618178) In general I was making homemade oven-baked ‘fries’ (thinly sliced par-boiled potato). I would often give in and allow myself ketchup or spicy mayo. I also went through some phases of doing homemade gnocchi, mashed potato, and faux-dauphinoise (thinly sliced, stacked, oven-baked potatoes with veg stock and a bit of butter).
As you can see, many people boiled their potatoes or used frozen potato products that were likely boiled in some way before freezing. But to be fair, this does not describe everyone. Some people did report mostly baking or roasting:
(58681391) I usually baked an entire 5 lb. bag of gold potatoes at 350 for 1.5 hours, for roughly three servings. I didn’t use oil when baking but would sometimes refry the baked potatoes into hash browns with about 1 tsp of avocado oil.
(70030447) My main method for eating potatoes, as I work from home, was to chuck a few russets in the oven for an hour after coating them in salt and pepper, then once they’re done I would cut them into two halves and eat those entirely. I found olive oil a hassle, and putting salt and pepper on the insides after they’re done was also too much hassle for me to want to bother doing everyday. Maybe I’d do that if I cooked them some other way.
Despite eating baked or roasted potatoes, neither of these people lost weight. The first saw no change at all, and the second gained 4 lbs. This is enough to show that baking or roasting is not enough to ensure weight loss.
But there may be other reasons these two didn’t lose any weight. 58681391 ate a lot of tomato and dairy, and got only about 38% of their calories from potatoes. 70030447 ate an unusually large amount of dairy (third most out of everyone) and got only about 20% calories from potatoes.
In any case, we still suspect that starting with whole, raw potatoes, and not boiling, soaking, or blanching them, might be important for causing potato weight loss. We didn’t make people roast or bake their potatoes in the original potato diet study, but maybe with +90% potato, it doesn’t matter.
It might have been an oversight not to ask people to roast or bake their potatoes for the half-tato protocol. If you’re trying it for yourself, probably don’t boil them or live off of frozen french fries.
Regression Analysis
To wrap up these correlational analyses, we fit some regression models to try to predict weight change from multiple factors at once. In all these models, we excluded the outlier who lost 17 lbs, participant 25348806, because we wanted to try to understand things that might have impacted weight change for the average participant, who did not lose so much weight.
One especially strong model included total dairy consumption (p = .007), total tomato consumption (p = .003), and their interaction (dairy * tomato; p = .035). This interaction had a negative sign, suggesting that tomatoes and dairy are slightly less than the sum of their effects. All three terms were significant predictors of weight change, and the model explained 23.7% of the adjusted variance in people’s weight change.
This was a much better fit than we expected, especially given the small sample size, and it provides more support for the idea that tomato and dairy consumption for some reason inhibit the potato weight loss effect. Note that this is TOTAL dairy and tomato consumption over four weeks, not average daily consumption, which provided a weaker fit.
This was not the best model we found, however. When you dummy-code the three potato protocols, and put them in a model with total tomato consumption and the two-way interactions, many terms are significant (for example, True Half-Tato condition * tomato sum is significant, p = .0004) and the model explains 37% of the variance in weight loss. We literally are not sure what to think of that, and are not sure how to interpret this result.
In any case, these are very simple models. It will be hard to squeeze more information out of just 37 observations, but if you have experience with more complex forms of statistical modeling, we encourage you to download the data and see if you can make more sense of it than we can.
Potatosis
Some people liked getting half of their daily calories from potatoes:
(23555212) This was cool! I have a newfound appreciation for potatoes.
Other people did not:
(28228309) Oh happy day. No more forcing myself to eat bland potatoes.
(81471891) Not super happy with my mindset about this diet. It’s currently “I *have* to eat 1 kg of potatoes per day!”, and feels a bit forced.
This is kind of striking compared to the absolutely rave reviews we got about the 100% potato diet, where most people said that they loved it. You’d think that eating 100% potatoes would be a bigger ask and a bigger pain than eating just 50% potatoes, but apparently not.
This makes us wonder if most people in this study never went into “potato mode”. In the original potato diet study, we found that after a day or two of eating potatoes, most people’s appetites waned, they didn’t want anything aside from potatoes, and they began to steadily lose weight. This seemed like a separate “mode” the body can be in, that both caused weight loss and made it easy to eat nothing but potatoes without major discomfort.
If something about the half-tato diet keeps people from going potato mode — the percent potato wasn’t high enough, the potatoes were prepared wrong, ketchup is a potato inhibitor, etc. — that would explain why people didn’t lose much weight, and why many people found it difficult to stick with even a mere 50% potatoes.
This is corroborated by a comment from one person who was also a participant in the original potato diet study, and says that they found half-tato very different:
(42475044) Overall this didn’t work anywhere near as well for me as the full potato. My weight over the last 8 weeks has largely stayed the same, whereas on the full-tato I lost 9 pounds in 3 weeks. I could definitely feel that the potatoes were helping me not gain weight, but I think my non-potato calorie intake was just too high for the potatoes to compensate for. On the full-tato diet I was able to eat as much as I wanted and still lose weight, but that doesn’t seem feasible for me on half-tato.
That said, at least one person on the half-tato diet did report signs that sound a lot like potato mode:
(21268204) Sweating at night, which I never do otherwise. Appetite low… Get full really fast even when eating non-potatoes … 2nd day in a row that it didn’t occur to me to eat until 4pm … Have not been hungry at all the last few days. The calories I did get were because I forced myself to sit down, mostly, with some potatoes
This participant lost only one pound over the first four weeks, but kept going and lost 3.5 lbs over eight weeks.
All this suggests that there might be a right and a wrong way to do half-tato. If you do it wrong, basically nothing happens, maybe you lose a little weight on average. But if you do it right, you go into potato mode, much like on the full-tato diet, and you start losing weight very quickly.
Let’s assume for the moment that there is such a secret magic switch (or set of switches) that can make half-tato cause rapid weight loss, and try to figure out what it is. If there is such a switch, then almost everyone on the full potato diet tripped it. All the case studies (like M) managed to trip it. The major weight-loss outlier in this study, and maybe some of the less major outliers, seem to have tripped it. Maybe they were doing something right that puts you in potato mode — so what would that be?
The extreme outlier (25348806) in this study give us a fairly detailed report of how she approached half-tato, saying:
I signed up for a spreadsheet for 52 weeks. I’m doing the diet and have had great success … Am female with 100 or so lbs to lose (now 30 down).
I first lost about 15 lbs doing a very loose version of potato by default after first reading your blog pre half tato experiment and have since lost another 15 beginning April 22 with starting half tato in earnest. I steam peeled yukon gold in batches in the Instant pot for 12-15 minutes at high/manual (depends on size, I try to get bigger but often its just medium available). Right out of the instant pot I add white vinegar which helps preserve color and appearance and tastes great later (more subtle than adding vinegar at mealtime) before cooling and fridge. I started eating a mix of cold and hot depending on if microwave is available (sometimes with mustard) but now I’ve settled into just hot (2 min microwave) with mainly salt. I try to have this 2-3 meals out of the day (2 medium or 1 big 1 smallish per meal). One of the 2 potato meals I may add one of: poached egg yolks; calf liver lightly sauted in butter (plus lingonberries and/or honey); or cooked ground beef (with 21 gun salute seasoning from trader joes and sometimes full fat sour cream), and possibly pepper or cholula sauce (rare), occasional oysters (fresh or canned). I don’t add ketchup (except once – when I went out and had beef fat fries at a steakhouse bar which did not seem to stall). I really enjoy the potatoes and look forward to them. I am not hungry but feel satisfied. I also have dairy – at least one glass of milk a day (either raw whole milk or 2% or whole conventional) – and a small amount of juice or lemonade. Some mornings I may have full fat yogurt with collagen and stearic acid (see fireinabottle.net) but not all mornings. I have some extra potassium as well as other supplements.
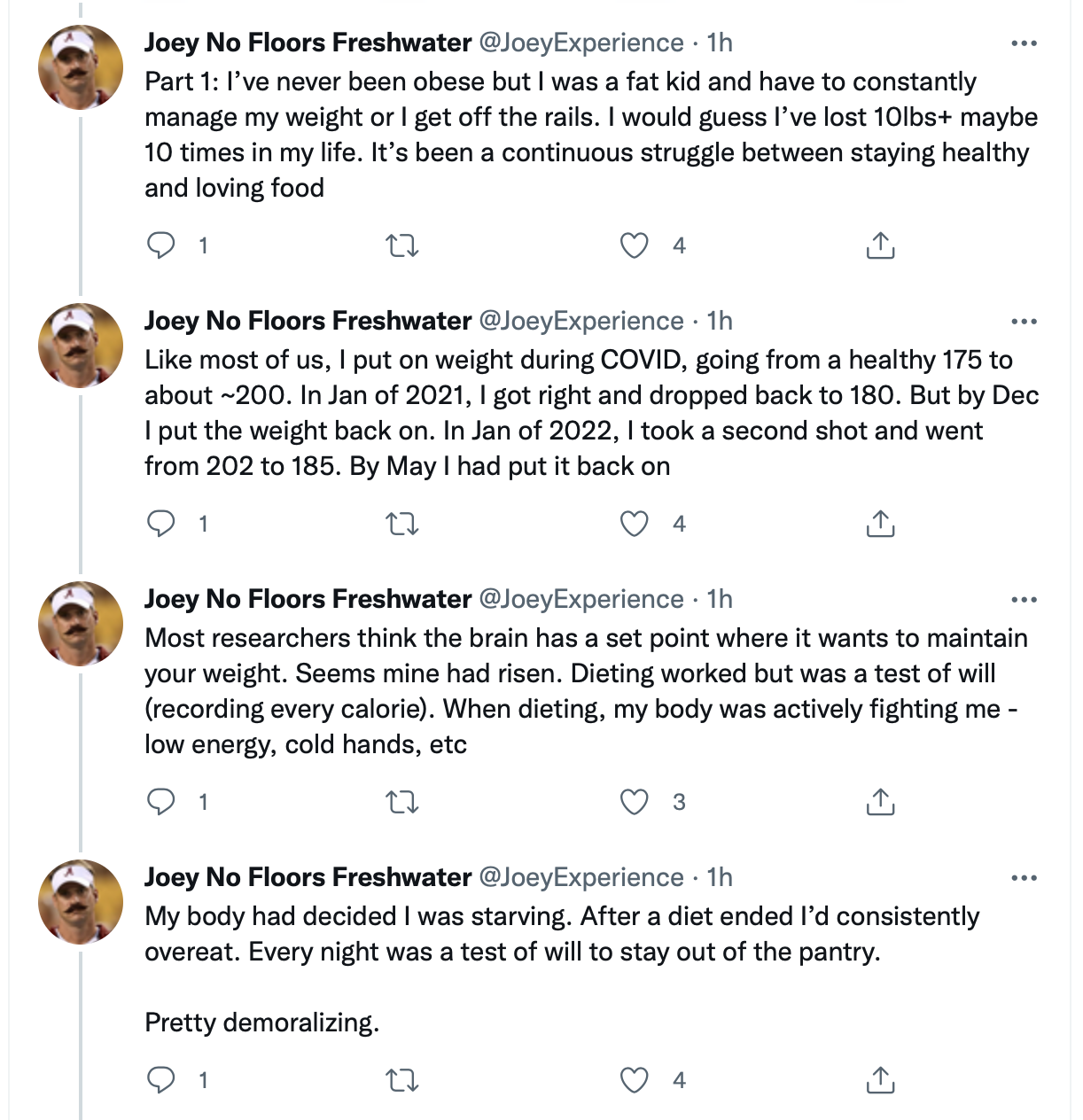
We love the level of detail, but it’s hard to know which of these elements are required to enter potato mode, if any of them are. But there are some features that this outlier and all the half-tato case studies (M, Nicky, and Joey “No Floors” Freshwater) share:
Nicky had a bit of ketchup, but everyone else either never or almost never had ketchup with their potatoes.
None of them avoided dairy
All of them mention eating meat and eggs
All of them used butter and/or oil
None of them ate boiled potatoes; their potatoes were generally steamed, air fried, microwaved, or baked
To us, this further supports the idea that at least part of the secret switch is eating not-boiled whole potatoes and mostly avoiding ketchup and tomato products. Dairy doesn’t seem to matter much, or at least it didn’t stop these people, and neither do various fats, meat, or eggs. Of course, it’s difficult to tell if there might be some ADDITIONAL element that they are all getting right. Are they all getting lots of magnesium or something? Hard to say.
Just in case it helps, here’s a closer look at the other people who lost relatively large amounts of weight on the half-tato diet:
Participant 26130773 lost the second-most over four weeks on half-tato, a total of 9 lbs. Overall he ate a good potato percentage, reporting 40%-60% most days, though on some days he only got 20%.
This participant left almost no notes and didn’t report his dairy or tomato intake, which makes it hard to figure out what he might have been doing right. But one thing that jumps out is that it’s clear he was eating lots of eggs. Here are his notes from the first three days of the diet:
5 eggs, potatoes for lunch (350 cal eggs. If I do 2 yokes 3 whites, 190 cal) Protein shake (120) for snack Turkey b patty, salad (600?)
5 eggs w 2 yolks, few bites turkey (225) Protein shake (120) Soup w meatballs (500)
5 eggs w 2 yolks (190) Protein shake (120) Normal dinner cheat (900) 2 drinks
Participant 56896462 lost the third-most over four weeks on half-tato, a total of 6 lbs. He had a very good potato percentage, 40% or 50% almost every day. He ate some dairy and some tomato, about 2 servings of dairy a day and 1 of tomato, on average. He also left very few notes, though we notice that he is in Italy.
Conclusions
The half-tato diet causes some weight loss in most people, but for most people, it is much less than half as effective as the full potato diet. If you really want to lose weight, probably go for the full potato diet instead, and try to get as close to 100% of your calories from potatoes as you can.
However, a small number of people do lose a lot of weight on the half-tato diet. This suggests that there might be some way to go into “potato mode” while on half-tato, if you do it right. If we could find out how to make this happen reliably, that would be pretty neat.
Our guess is that it involves some combination of:
Baking, steaming, microwaving, or roasting whole potatoes instead of boiling them or using pre-boiled frozen potato products
Avoiding tomato products, especially ketchup
Getting enough of something else, possibly something found in eggs, meat, or dairy.
We should note that this list is largely based on circumstantial and/or correlational evidence. We do worry that ketchup might be a potato-blocker, but the evidence is not yet all that strong. That makes all of these guesses good subjects for future experiments.
You could design a large trial to answer these questions — randomly assign 100 people to do half-tato with ketchup and 100 people to do half-tato without — but you might need a very large sample size to be able to detect a difference. And while we’d love to see more community trials, it may not be practical to do multiple trials of several hundred people each, one after the other, to try to chase down whether each of these things makes a difference. That seems like it would take forever and be a lot of work.
So instead, another option would be for individuals to test these guesses as a self-experiment, which could provide very strong evidence, and might be able to provide it quickly.
For example, let’s say that Gary is a fellow who is happily losing 2 lbs a week on the full-tato or half-tato diet. Whatever makes potato mode happen, Gary has found it, even if he doesn’t know what he’s doing right.
Now Gary can test individual switches to see if they turn potato mode off. For example, he can randomly assign some weeks to be ketchup weeks, where he always has ketchup with his potatoes, and other weeks to be no-ketchup weeks, where he religiously avoids ketchup and all other tomato-based foods.
If Gary’s weight loss always stalls on ketchup weeks, but continues humming along on no-ketchup weeks, that’s a pretty clear sign that avoiding ketchup is one of the switches to make the half-tato diet work. If the randomization makes no difference, that’s a pretty clear sign that ketchup doesn’t matter, at least not for him.
You can imagine a similar design for anything else. Gary could randomly assign some weeks to try only boiled potatoes, and other weeks to try only baked potatoes, and see if it makes any difference.
We doubt things will be this simple — it’s quite possible that one brand of ketchup kills the potato effect, while another brand has no impact — but we won’t know until someone has tried. It might take several weeks to pick up a clear signal, but anyone who is able to get a potato diet working for them can test any of these switches out for themselves.
All we ask is that if you try something like this, please publish your results online, regardless of how it turns out. We’re very curious to know what will happen!
Closing Notes
Some people have gone for more than eight weeks on half-tato, and we plan to analyze their results at some point in the future. It will be a small sample size, but we are excited to have some more case studies. So stay tuned.
If you are interested in doing an N=1 experiment about these ideas and want our help designing a protocol, please feel free to contact us.
If you would like to be notified of future stupid studies, or if you want to keep up with our work in general, you can subscribe to the blog by email (below), or follow us on twitter.
And if you feel like reading this post has added a couple of dollars’ worth of value to your life, or if you have lost weight as the result of our research and you think it improves the quality of your life by more than one dollar a month, consider donating $1 a month on Patreon.
Thanks for going on this journey with us.
Sincerely, Your friendly neighborhood mad scientists, SLIME MOLD TIME MOLD
In the old days, psychology was dominated by the school of behaviorism.
Behaviorism taught that mental states like thoughts and feelings are unworthy of study, and possibly don’t exist.
Behaviorists also thought that animals are born without anything at all in their brains, that the mind at birth is a blank slate, and that everything an animal learns to do comes from pure stimulus-response learning built up over time. Turns out, this is wrong.
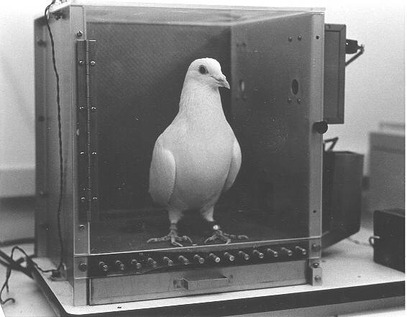
At some point in the 1950s, a guy named John Garcia was irradiating Sprague-Dawley rats for his job at the U.S. Naval Radiological Defense Lab, like you do, when he noticed something weird. The rats who had been exposed to low levels of gamma radiation were eating and drinking less than usual, and groups that had been exposed to radiation the most times ate and drank the least.
Garcia thought that the rats might be learning to associate their food and water with the nausea from radiation exposure. After all, rats have no concept of ionizing radiation, so from their point of view, they were going about their day as normal when they suddenly started feeling nauseous for no clear reason. They might reasonably wonder if it was something they ate. In particular, he noticed that the rats wouldn’t drink out of the plastic bottles they were used to, but were happy to drink out of unfamiliar glass bottles. Garcia thought that maybe the plastic bottles gave the water a particular taste that the rats had learned to avoid.
So in a series of experiments, Garcia tried exposing rats to different kinds of stimuli to see what they would learn. He discovered two surprises that called the whole behaviorist concept into question.
First, he discovered that if a rat was exposed to radiation (making it nauseous) after encountering a new food, it would quickly learn to reject the food, even if the radiation came hours later.
This contradicted the understanding at the time of how conditioning worked — behaviorists thought that you had to present the unconditioned stimulus (nausea) immediately after the conditioned stimulus (the new food), or the animal wouldn’t learn to associate the two. But Garcia found that learning could occur even if the rat got sick well after eating a new food.
Rats would instantly associate nausea with whatever food they had most recently eaten, and had no problem doing so. If he made them sick after giving them Cheetos, they would learn to reject Cheetos forever. But the rats simply could not learn to associate their nausea with any other kind of stimulus. It didn’t matter if the stimulus was bright lights, or an annoying buzzer. No matter how many times Garcia flashed lights at them, the rats never learned to associate their nausea with the lights.
Everyone knows it’s mice that like cheetos, anyways
On the flipside, when he gave the rats electric shocks instead of exposing them to radiation, they would learn to be afraid of the lights and sounds. But no matter how many times he shocked them after eating, the rats would never learn to associate food or water with getting shocked.
This was another big pie in the face of behaviorism. Learning was supposed to be purely stimulus-response, and you were supposed to be able to teach an animal to do just about anything by pairing a behavior with the right reward or punishment. But Garcia’s rats seemed to be hard-wired to associate nausea (from radiation) with what they ate or drank, and similarly hard-wired to associate pain (from electric shocks) with what they saw or heard, and not to associate these things with anything else.
This was confusing to the behaviorists, but makes perfect sense if you think about evolution for even one second. In the real world, rats become nauseous when they eat spoiled food, so it’s important for a rat to associate nausea with things they recently ate. Any rat that doesn’t learn this will be dead, so eventually all rats are born prepared to make these food-nausea associations. Even though Garcia’s rats had been born in a laboratory and had never eaten a bit of ham left out in the sun for too long, they still came with an overwhelming bias to associate a feeling of nausea with whatever they most recently ate.
Similarly, pain is associated with sights and sounds, like the sight of an owl or the sound of a fox; or specific locations, like parts of the forest where predators are common. So rats are born ready to associate pain with things like weird noises or flashing lights. The idea that pain might be related to food, on the other hand, never crosses their minds.
…[cats’] lack of trainability apparently has an exception, Bradshaw states: food can trigger learning of powerful associations even hours after consumption. This would make sense as an anti-bad-food defense, but unfortunately, this is yet another maladaptation in the modern context: “…this mechanism occasionally has unexpected consequences: a cat that succumbs to a virus may then go off its regular food even after it has recovered, because it has incorrectly associated the illness with the meal that happened to precede it.”
More generally this is called conditioned taste aversion, and it occurs in most mammals — though maybe not vampire bats, since they eat only one thing that never spoils, and being put off their food would be a guaranteed death sentence.
(Some researchers did a version of Garcia’s study where they compared vampire bats with closely related species of bats that eat more than one thing, and while the other bats learned to avoid new flavors that were paired with nausea, vampire bats didn’t learn to associate new flavors with nausea when they were fed different kinds of flavored blood. Just imagine being that researcher on a first date; “Oh, what do I do at work? Yeah, I’m the guy who injects vampire bats with a 1% weight/volume lithium chloride solution to make them nauseous, it’s not much but it’s a living!”)
II.
Humans are also mammals, so we might have the same tendency. Maybe when we feel nauseous, or sick, or even just kind of weird, we assume it’s something we ate or drank.
Wikipedia thinks this is the case, claiming, “even something as obvious as riding a roller coaster (causing nausea) after eating the sushi will influence the development of taste aversion to sushi,” but doesn’t offer any citations. We suppose you could run this study on your own with a few sushi meals and a season’s pass to INSERT LOCAL THEME PARK.
People often suspect that their chronic illnesses have food triggers, different kinds of food or drink that will bring on an attack or generally make them feel like crap. But if our brains are hard-wired to pick out food-based explanations for feeling ill, maybe we tend to latch onto the idea of some food trigger causing our illness, even when food has nothing to do with it.
When our ancestors felt nauseous, it was usually because they had eaten the wrong kind of frog, so we come with a strong bias towards assuming that a random feeling of sickness is connected to something we ate. We don’t assume it has anything to do with the awesome glowing rocks we found in that sweet cave.
Such a cool rock, right? Oh hold on I have to lie down I feel terrible, must have been the goat’s milk I had for lunch
This worked well up until 3000 BC, but since then humans have discovered and invented lots of new things that can make you sick, most of which are not foods.
In general this should make us more skeptical of food triggers (and food-related triggers like packaging), especially if your chronic complaint is anything related to nausea, anything that feels like an illness, or anything digestive.
Food can still make you sick, and there are for sure some real food triggers out there. But the lesson here is that your instincts will tell you that your random sickness is caused by what you ate, even if it’s actually caused by something completely different. If you were one of Dr. Garcia’s rats, you would never have guessed that you were being hit with gamma radiation. You’d be all like, “it must be some chemical in those nasty plastic bottles.”
The biggest limitation of an N=1 experiment is external validity. If you run enough trials on yourself, you can show that some intervention does or doesn’t have an effect on you to basically any degree of certainty that you want. But this will never provide much evidence that the same intervention will have the same effect, or any effect, on anyone else.
People are all human and have roughly the same human biology, it’s true. In the higher animals, decapitation is more or less guaranteed to be lethal; people generally like eating sugar and hate eating asphalt. But once you move beyond the fundamentals of biology, most other bets quickly are off.
An unspoken assumption of the self-experiment discussion (including our posts on the subject) is that there are exactly two kinds of research — self-experiments, and large trials. These occupy the sample size slices of N = 1 and N ≥ 30, respectively. The self-experiment and case study are assumed to be a single subject; and with few exceptions, most people don’t trust a survey or RCT with anything less than 30 participants.
But there are two problems with this perspective. The first is that this is a false dichotomy. There isn’t a point where N = 1 turns into N = small, and there’s no sample size where you go from having a collection of case studies to having a trial. Going from N = 29 to N = 30 does nothing in particular, and there is no other threshold that stands out as being at all distinct (except N = 0 to N = 1, of course). A bigger sample size always means more information and better external validity, with no discontinuity.
The second problem is that if N = 1 is at all good (and we think that it is), then N of small has to be better.
Anything that is good with an N of 1 will be better with an N of 2-10. With N of small, you get more data, more quickly. One person doing random daily trials over the course of a week will create 7 data points. Three people doing random daily trials over the course of a week will create 21 data points. Small-group analysis is a little more complicated, but the data can be handled by a standard linear mixed model (here’s an example that involves dragons).
With N of small, you get more diversity of participants and more diversity of responses, quickly drawing the fangs from the problem of external validity. You will be able to get some sense of whether the intervention works differently for different people. If you have five participants, it will be easy to see if they are all responding the exact same way, if they are responding somewhat differently, or if some of them are having huge responses while others feel nothing at all.
The only question is one of cost. Because while the biggest limitation of N = 1 is external validity, the biggest benefit is that it’s cheap in important ways. With N = 1, you don’t need anyone’s permission to start your study — you can just go do it. You don’t pay any coordination costs, costs which are easy to miss up front but can be quite a drag if you’re not careful. These factors help make self-experiments cheap.
But we think scaling up is usually worth it — or at least, once you have some promising N = 1, scaling to N of small usually makes sense. It’s the logical next step. And since there’s no real distinction between a single case study, a small collection of case studies, and a trial of 100 people, it’s also the logical next step on the path towards an RCT or other large trial.
So while this series has focused on true N = 1 self-experiments, the real wins for the future may be in N = 2-10 studies where people grab a couple of friends and run a self-experiment together. Remember kids, friendship is the most powerful force in the universe.
And it’s not at all unprecedented, since this is how we approached our community trials; we looked at a couple of case studies, and then used N of small to do the pilot testing.
For the potato diet, we started with case studies like Andrew Taylor and Penn Jilette; we recruited some friends to try nothing but potatoes for several days; and one of the SMTM authors tried the all-potato diet for a couple weeks.
For the potassium trial, two SMTM hive mind members tried the low-dose potassium protocol for a couple of weeks and lost weight without any negative side effects. Then we got a couple of friends to try it for just a couple of days to make sure that there weren’t any side effects for them either.
For the half-tato diet, we didn’t explicitly organize things this way, but we looked at three very similar case studies that, taken together, are essentially an N = 3 pilot of the half-tato diet protocol. No idea if the half-tato effect will generalize beyond Nicky Case and M, but the fact that it generalizes between them is pretty interesting. We also happened to know about a couple of other friends who had also tried versions of the half-tato diet with good results.
We think that in all of these cases, N of small was much more convincing than N = 1 would have been. With two people, it’s much less likely that the effect is a fluke. Even if it works for one person and not for the other, that’s still evidence that we shouldn’t expect the effect to be entirely consistent; we should expect more ambiguity. And for something where the risks are unclear, like with potassium, two people going through without any side-effects is much more reassuring than one.
Peter has a bad reaction to melons. Every time he eats melon, he gets sick right away, and he often throws up.
We can say that Peter’s reaction to melon has low latency. When it happens, it happens right away. No waiting about.
Mark also has a bad reaction to melons. But because of a complex series of biochemical interactions, when Mark eats melon, he doesn’t get sick right away. He gets sick about three days (72 hours) later, when he suddenly starts to feel very ill, and then often throws up.
We can say that Mark’s reaction to melon has high latency. It happens, but it always takes a long time to kick in.
Peter and Mark have basically the same reaction to melon. Both have the same symptoms — nausea, sickness, and vomiting. Both reactions happen for sure every time — they are both equally reliable. The only thing that’s different is the latency.
b. Different and the Same
Though their reactions are nearly identical, Peter and Mark end up with very different experiences of their sensitivity.
Peter quickly learns that melon is a trigger. After all, he gets sick right away. He just makes sure to avoid melon and goes about his life with no additional air of mystery.
Mark, on the other hand, is plagued with random, crippling nausea. He sometimes gets sick, and it always seems to be for no reason. This is because it’s hard to remember what you were eating exactly 72 hours ago (for example, take a moment to try to remember what YOU were eating 72 hours ago). So for Mark, the connection is very obscure. He may never figure it out.
Both of these relationships would become equally obvious in a self-experiment. As long as you were tracking melon consumption and looking for relationships over a long enough time frame, you would see that Peter gets sick right after every dose of melon, and Mark gets sick exactly 72 hours after every dose of melon.
Perfect 100% reliability would make this pretty obvious once you noticed it. You don’t need a huge sample size to pick up on a relationship that is 100% reliable, which is why Peter quits melons after getting sick just a few times.
The big difference is whether the relationship jumps out at you or not. Low-latency relationships are obvious; the close proximity of cause and effect highlights the correct hypothesis and draws immediate attention to the relationship, where it can quickly be confirmed. Peter can just eat more melon and immediately get corroborating evidence if he wants to confirm his theory. The relationship is intuitive; you know it when you see it.
c. Cause and Effect
High-latency relationships are much harder to spot, even if they are equally reliable. The separation of cause and effect means that the connection may never come to mind.
To even be able to pick up on this in a self-experiment, you would have to know in advance that you should be tracking how much melon you are eating. And this is the hard part. The hard part is not demonstrating the relationship. At 100% reliability, that’s easy. The hard part is picking up on what to track.
This is somewhat in contrast to our normal concerns in research. Normally we worry about sample size and the quality of our measures. But Mark doesn’t need a big sample size. He doesn’t need any measures other than “got sick” and “ate melon”. All he needs is to consider melon as a possible cause of his nausea, and to consider looking for relationships with a latency of at least 72 hours. Easier said than done.
d. Reliability in Real-World Relationships
Of course, most real-world relationships are not 100% reliable. Few things work every time. But it’s concerning how a little latency can hide an otherwise blatant relationship, and it makes us wonder how many connections we all miss because of relatively small delays in onset.
Zero latency (eat melon, immediately puke) is easy to figure out. These relationships become obvious after just a few trials.
In comparison, 72-hour latency is very hard to figure out. Most people are not looking for relationships with such a long delay, and even if you were, you would be hard pressed to figure out the cause.
You can’t just keep a food journal and look 72 hours back — you don’t know how long the latency is, so you don’t know how far back to look! And if the latency varies at all (e.g. always between 60-80 hours later), it gets even harder.
This makes us wonder how much latency we can handle before connections stop being obvious. It may not take much. Coffee -> heartburn with an hour delay, that seems pretty doable. We think you would figure that one out pretty quickly. But with a four hour delay? Eight hours? Twelve? This would be much more difficult. It would start to look more like, “heartburn around dinnertime / going to bed, especially on weekdays”. That sounds hard to puzzle out.
Latency also makes it harder to get a big sample size. With a latency of less than 5 minutes, Peter can easily do eight trials (eat some melon and face the consequences) in a single day. Mark can’t do that. He has to wait 72 hours to get the results from his first trial, except it’s worse than that, because he doesn’t know how long he has to wait for the results to come in.
If he wants to make sure not to cross the streams, he needs to devote three whole days (though again, he doesn’t actually know in advance how much time he has to dedicate) to each trial, so he needs 3 * 8 = 24 days to do the same number of “eat melon and find out” trials that Peter can easily do in an afternoon, if he’s willing to get sick that much in a single day.
II. Half-Life
a. Creamer
Jo has a bad reaction to one of the additives in her office’s tiny cups of dairy creamer (henceforth: “creamer”). Every time she uses one of the tiny cups, she gets very tired about 30 minutes later. Fortunately, Jo’s kidneys happen to handle the additive really well, and two hours after she takes the creamer, she has cleared all of the additive out of her system, and stops feeling unusually tired.
We can say that the additive has a short half-lifein Jo’s system, and that the symptoms (fatigue) have a short half-life as well. They don’t stick around for long, things quickly go back to baseline.
Lily works in the same office and has the exact same reaction to the same additive in the office’s tiny cups of dairy creamer. Every time she uses one of the tiny cups, she gets very tired about 30 minutes later. But through a random accident of biology, Lily’s body doesn’t clear the additive from her system nearly as quickly as Jo’s does. The additive sticks around for a long time, and Lily keeps feeling tired all week. If she takes some creamer on a Monday, she’s just getting over it on Sunday afternoon.
We can say that the additive has a long half-lifein Lily’s system, and that the symptoms (fatigue) have a long half-life as well. They stick around for a long-ass time, and it takes forever for her to feel normal again.
b. Puzzling it Out
Much like a long latency, a long half-life makes this problem much harder to puzzle out, even when the two cases are otherwise identical.
Jo has it easy. If she comes to suspect the creamer, she has a lot of options. She can try taking creamer some mornings and not other mornings. She can try taking the creamer at different times of day and seeing if the fatigue also kicks in at different times. She can even take the creamer multiple times in the same day. Since the symptoms clear out after just two hours, she’s quickly back to baseline and is ready for another trial. If she wants to compare different brands of creamer to see if there’s a difference, she can get a pretty good sample size in a weekend. It’s easy for her to collect lots of data.
Lily has it really hard. If she comes to suspect the creamer, she is in a real bind, and most of the traps are invisible. If she tries taking the creamer some mornings and not other mornings, her results will be a mess, because as soon as she takes it one morning, she is fatigued all week. It will look like the creamer has no effect at all, since on days when she doesn’t take the creamer, she is still fatigued from any creamer she took in any of the previous seven days. A day-by-day self-experiment would show no effect, even though this is totally the wrong conclusion.
To detect any effect, Lily needs to test things in blocks of weeks, instead of blocks of days or hours. Each Monday, either take the creamer or not, and see how tired she is that week. But you can see how hard it would be for her to figure out this design — how is she supposed to know in advance that she needs to study this problem in blocks of a full week? She has a lot less flexibility; you might say that her research situation is much less forgiving.
Half-and-Half-Life
Even if Lily does pin down the right research design, it still takes her much longer to get the same amount of data. Randomly assigning creamer or no creamer each morning, Jo can get 28 data points in four weeks, which is enough data to detect a strong relationship if there is one. Meanwhile, in four weeks Lily would get only four datapoints, not enough to be at all convincing.
If the relationship is weaker (e.g. only a 50% chance of becoming fatigued), things are even worse. Jo can get a sample size of 100 or 200 days if she has to; it would be a pain, but she could make it happen. But for Lily to get a sample size of 100 weeks would take two years.
c. Thought it Worked for a While 🙂
Lots of people try something, feel like it works great, and then later when they do a more rigorous self-experiment or just keep trying it, they feel that the effect wears off. Must have just been excitement over trying a new thing.
For example, back in early 2020 Scott Alexander put out a report describing his experience with Sleep Support, a new (at the time) product by Nootropics Depot. His sleep quality isn’t great, so he decided to give this new supplement a shot, and reported miraculous results:
The first night I took it, I woke up naturally at 9 the next morning, with no desire to go back to sleep. This has never happened before. It shocked me. And the next morning, the same thing happened. I started recommending the supplement to all my friends, some of whom also reported good results.
“I decided the next step was to do a randomized controlled trial,” he says. To make a long story short, the RCT found no difference at all in any measure of sleep quality. “My conclusion is that the effect I thought that I observed – a consistent change of two hours in my otherwise stable wake-up time – wasn’t real. This shocked me. What’s going on?”
Scott chalks this up to the placebo effect, which is certainly possible. But another possibility is that Sleep Support did work great at first but was no longer detectable (for whatever reason) by the time he set up the RCT. Obviously if this is true, it would be hard to study; but it does perfectly match Scott’s experience, which is otherwise (as he says) shocking and somewhat confusing.
If you have any experience with chronic illness or biohacking or anything similar, then you know that “thought it worked for a while” is a very common story. When this happens, the assumption is usually that you were fooling yourself the first time around. But consider:
Vitamin C cures scurvy, so if you have scurvy, the first few doses of vitamin C are great! But after that, vitamin C has basically no effect, because you no longer have scurvy. You have been cured. Looking at this data (huge increases in wellbeing on the first few days, but after that, nothing), the research team concludes that the original reports were somehow mistaken.
No! It’s just that the vitamin C helped and then it had done all it could! It had a huge effect! That effect was just all up front!
This exact scenario should pop up all over the place. If you are iron deficient, the first few doses of iron will have some effect. After that, they will have no effect. If you are B12 deficient, the first few doses of B12 will have some effect. After that, they will have no effect. Et cetera.
This is because the body is able to keep reserves of all of these substances. As long as you’ve been getting enough vitamin C, you can go for 4 weeks without any vitamin C at all before you start getting scurvy (in reality it usually takes more like 3 months, because most people don’t go entirely cold turkey on vitamin C). Same goes for iron and B12 — your body is able to keep reserves of these substances, so as long as you get enough, you should be set for a while.
To put this back in the terms of this essay, we would say that these positive effects have a long half-life. Positive effects with a long-half life face exactly the same issues as negative effects with a long-half life — you have to make sure you take the half-life into account when designing a study, and use long enough study periods, otherwise your data will be confused and misleading.
This same point applies to a lot of treatments, actually. Assuming you have an infection, antibiotics will show a big effect up front and then nothing after that. But we don’t take this to mean that antibiotics have no effect, oops we thought it worked for a while, guess we were wrong.
This isn’t a problem for things with no reservoir. For example, as far as we can gather, zinc isn’t really stored in the body long-term. So most effects of zinc will (probably) have a short half-life. If you need more zinc, you can just take it on a given day and see the effects.
Supplementing anything with a large reservoir (or other positive effect with a long half-life) may not be suitable for a self-experiment, because it will show a strong effect in the first few days and no effect after that. Aggregated over 30 days or whatever, this will look like no effect or a weak effect. Clearly this is the wrong interpretation.
And the longer you run the self-experiment for, the smaller the effect will appear! If you do a 10-day self-experiment with antibiotics, and they have an effect on the first two days, then you will find that this looks like 2/10 days show an effect, which will probably average out to a small effect. But if you kept going for 100 days, you would see that 2/100 days show an effect, which will average out to basically no effect at all.
This is the opposite of our normal assumption about sample sizes, that a larger sample size will always get us a more meaningful, accurate estimate. This assumption simply isn’t true if we’re dealing with a treatment that has a long half-life.
So consider the half-life of positive effects too.
III.
Broadly speaking, triggers have some delay in the onset of their symptoms, and those symptoms stick around for some span of time.
Having a high latency or a long half-life makes a relationship much harder to notice, and harder to study. Having both, it gets even worse.
Perhaps Bob is allergic to dairy, or whatever. It gives him hives, but with a latency of two days, and they persist for four days. Bob will be walking around with random hives, and not much hope of finding out why.
He might come to suspect the true cause if he happens to cut out dairy for a while and the hives go away for good. But if someone challenged him on this — or if Bob, being a good scientist, decided he wanted to run a self-experiment to demonstrate the hive-causing effect — he would be hard pressed to get convincing formal evidence.
Bob wouldn’t know in advance to look for a latency of two days and persistence of four days. If he did something reasonable, like randomly assign each day as dairy or non-dairy, the results would look like zero effect. On most days when he took no dairy, he would have hives anyways, because of the long half-life. On most days when he did take dairy, he would also have hives, because they stick around so long. The few “no hive” days would be in the random periods where he hadn’t had any dairy several days ago; but those days might well be days when he was assigned to drink dairy. So it would look like a wash, even though it’s actually a very reliable relationship.
Bob would have to do something that seems totally unreasonable, like structure the trial in 6-day segments to account for these delays. If he did this right, the 2-day wait and 4-day stay would become entirely obvious. But how is he supposed to know in advance that he has to use this totally weird study design?
People like to argue about whether obesity is a disease. Does it require treatment, or is it more of a social problem? But obesity isn’t a disease. It’s clearly a symptom.
Think about it like this. Fatigue is a symptom, and it’s a symptom of many things. Fatigue can be a symptom of everyday decisions — you can be fatigued because you stayed up until 3 AM last night playing Octodad: Dadliest Catch. It can be a symptom of substances, like alcohol or Benadryl. It can be a symptom of conditions, like anemia or concussion. And fatigue can be a symptom of diseases, like mononucleosis, Parkinson’s, or lupus.
Similarly, a person can be obese for a number of different reasons. Obesity is a symptom of many different conditions. You can be obese because of a brain injury. You can be obese because of a thyroid issue. You can be obese because you’re taking a drug like haloperidol or olanzapine. And while there’s still a lot of dispute over the source of the global obesity epidemic, you can be obese because of whatever cause(s) are causing that.
II.
Things get confusing when you try to treat a symptom like a disease.
Think about fatigue. If your friend is tired from playing video games until the wee hours of the morning, the correct treatment is for them to play video games while pretending to fill out spreadsheets at work, like a normal person. If they’re fatigued from drinking merlot or taking Benadryl, the only real option is to have them wait until the drug wears off (or take an upper, but that’s not really recommended). If they’re anemic, then they need to get more iron. Et cetera.
Similarly, we don’t know how to treat the general obesity we see in the obesity epidemic. But we do have treatments for obesity caused by thyroid disorders or brain tumors. And we shouldn’t be shocked if treatments that work for obesity caused by thyroid disorders don’t work for the obesity caused by brain tumors, or don’t work for the widespread obesity we see today.
Because a symptom can have many different causes, just looking at the symptom won’t always tell you the cause. And if you don’t know the cause, then you may not know the right treatment, because you don’t know the etiology; you don’t know how the cause connects to the symptom, at what points you can intervene, and what kinds of interventions might be helpful.
This is pretty bad — even when there’s a finite list of possible causes, it’s hard to look at a symptom and figure out which of its causes are responsible.
III.
Many chronic illness symptoms are nonspecific. Per Wikipedia:
Nonspecific symptoms are very general and thus can be associated with a wide range of conditions. In other words, they are not specific to (not particular to) any one condition. Most signs and symptoms are at least somewhat nonspecific, as only pathognomonic ones are highly specific. But certain nonspecific signs and symptoms are especially nonspecific and especially common. They are also known as constitutional symptoms when they affect the sense of well-being. They include unexplained weight loss, headache, pain, fatigue, loss of appetite, night sweats, and malaise.
This means that people who are diagnosed with the same chronic illness could have similar experiences, similar symptoms, with entirely different causes. If you have headache/pain/fatigue, you might reasonably assume that someone else with headache/pain/fatigue has the same illness, and that it was caused by the same thing. You might assume that the same treatments will work for both of you, that your illness would have the same cure.
But headache/pain/fatigue are all nonspecific — they can all be caused by a zillion [sic] different things. So someone who shares your exact symptoms may have the exact same experience but for totally different reasons. If this is the case, the treatments that work for one of you may not help at all for the other.
(Even worse, palliative treatments will tend to work for both of you, since they treat the symptoms directly, and this will make the two conditions seem even more similar. But curative treatments that work for one of you won’t work for the other, since your conditions have different root causes.)
Let’s consider migraines. Migraines can definitely be caused by hormones. Some people have migraines only during certain parts of their period (about 7-14% of women, according to Wikipedia), or only when pregnant. Migraines can also be caused, or at least partially caused, by triggers like stress or certain foods.
But there are also people who get random mystery migraines on a regular basis, with no apparent trigger. Presumably these are caused by something, but it’s not something obvious like stress or hormonal cycles or being pregnant. So clearly migraines are a symptom, not a disease — they can be caused by several different things.
All this to say that finding the “cause” of migraines may be the wrong framing. There may be no more single cause of migraines than there is a single cause of car accidents. Some accidents happen because the driver wasn’t paying attention (and many people think of this as prototypical). But some accidents happen because the road is icy. Some accidents happen because the driver had a seizure and lost control of the car. Some accidents happen because the vengeful spouse of the man you killed in El Paso 15 years ago has finally tracked you down and cut your brake lines.
Not that we would know anything about that! We’ve never been to El Paso, officer, we swear.
There is no single cause of car accidents. They are more like a symptom. All car accidents look much the same — broken glass, tire marks, people yelling. Most car accidents have similar proximal causes — unless it was an intentional ramming, it happened because someone lost control of their vehicle. But despite these apparent similarities, car accidents can have wildly different original causes. They happened for different reasons.
Consider chronic fatigue syndrome (CFS). Most people assume that CFS is a disease, and that everyone with CFS has it for the same reason, that there is a single cause. But maybe CFS is more like a symptom (obviously “syndrome” is literally in the name). If so, the search for the “cause” of CFS is a mug’s game, since it is caused by many different things. If you go around assuming there is one cause of CFS, one etiology, you are going to end up very confused.
Or consider irritable bowel syndrome (IBS). Most people seem to be aware that IBS is not really a single diagnosis, and probably is a term used to describe all sorts of different, unrelated things. E.g. “Some people just have trouble with their stomachs. When they have trouble and we don’t know what is causing it, we just call it IBS. So you have IBS.” Even so, the label kind of implies that there is a similarity of some sort, and suggests that maybe there will be some similarity of treatment and of cure. But this may be misleading.
If nothing else, the shared label means that all these people are likely to end up in the same groups or the same communities “for people with IBS”. If someone makes a post like “this treatment cured my IBS”, you can be sure other people will respond with, “well it didn’t cure *my* IBS”. This is guaranteed to be the source of a lot of confusion.
We think that most unsolved chronic illnesses are probably like this — most of them are probably different diseases with different causes that happen to look very similar.
Compare it to the anthropic principle if you like — diseases that present in a consistent way and have a single cause are easy to figure out, so they tend to be cured and don’t tend to be on the list of unsolved chronic illnesses. But diseases where a number of very different causes present very similarly will be quite hard to figure out, and are likely to remain mysterious for a long time. So things that are unsolved and have been unsolved for a while are more likely to have multiple causes.
(Though even simple illnesses with precise single causes, like scurvy, can be devilishly difficult to figure out, so take this argument with a grain of salt.)
IV.
Single-subject (aka N=1) research can be really powerful. But when it comes to cases like this, you have to be very careful. Even if you do a very rigorous single-subject experiment, and provide strong evidence that some treatment works for you, you’ve only really provided evidence that it works FOR YOU. It may not work for anyone else.
If the treatment that works for you doesn’t work for most other people with your diagnosis, that’s actually somewhat informative. We can see why some people would find it discouraging, but it suggests that the illness you have “in common” is actually two different illnesses, or at least two substantially different presentations. That means it gets us one step closer, a small step but a step even so, to figuring out what is going on with your illness, and maybe getting a cure or treatment for everyone.
If you end up with Treatment A that works for 20% of people with your condition, and Treatment B that works for 50%, and there’s basically no overlap, you’re off to a great start. You can start looking for anything that the Treatment A people have in common that’s never found in the Treatment B group, and vice-versa. If you find something (“holy cow, everyone who liked Treatment A has Irish heritage!”), you can start directing people to try the treatment that’s most likely to work for them.
Even if you find nothing in common within the groups, you’re still in good shape. There are only two treatments, and we know that Treatment B works for more people. Newcomers can start by trying B, and if that doesn’t work, they can try A next. If neither work, then they are in the other 30% with no discovered treatment. But it’s still progress in general, and you can start putting your efforts towards finding treatments C, D, E, etc.
It may be tempting to jump ahead and start looking for differences now, before we have treatments that distinguish between various groups, and there is some merit in this idea. If we find that half of people with IBS tend to have bloating with no reflux, and the other half tend to have reflux with no bloating (or whatever), that’s a pretty interesting sign, and will probably end up being useful.
But this approach doesn’t usually seem to work.[1] Probably this is because clustering by symptoms isn’t useful; or when it is useful, it will already be obvious. Different causes can present with identical symptoms, as we’ve been discussing. But IDENTICAL causes can also sometimes present with DIFFERENT symptoms! There’s no royal road, no way to cut this knot for sure. You just have to be careful.
The real enemy here is the confusion (lit. fusion together of different things; “(transitive) To mix thoroughly; to confound; to disorder.”). Talking about “having CFS” or “having IBS” is handy, but when it comes to diagnostics, more detail is better. You may be surprised to discover that someone with the same diagnosis as you has almost nothing else in common. And even when you have every symptom in common, don’t confuse this for a common cause. Your friend may also have migraines, but don’t be shocked when the thing that worked for you doesn’t work for her.
Remember that car crashes all have similar presentation. In true diagnostic fashion, they usually show three or more of the following symptoms: broken glass, injured driver(s), skid marks, bent fenders, police on scene, plastic debris on the road, etc. Take two Geico and call me in the morning.
it’s ok, this lizard is a doctor
If you only did an analysis of symptoms, you might think that all car crashes have the same cause. An analysis of symptoms would suggest just one group. But we know that’s not the case — car crashes can happen for many different reasons, and even car crashes with very different causes will usually have very similar symptoms.
Maybe if you are a genius detective and you know just what to look for, you can tell them apart — maybe a car crash caused by a seizure will show signs of uncontrolled driving well before the point of impact, while a car crash caused by excessive speed will have longer, straighter skid marks on the blacktop. But you certainly won’t be able to discover the different causes of car crashes by going down a checklist of “was there broken glass?”, “were there skidmarks?”, “were the drivers injured?”, etc.
If you add in criteria like “how long were the skidmarks?” you might get closer. But you’d have to understand the causes well enough to add that question in the first place.
ENDNOTES:
[1]: If you know of any examples of looking at a disease, looking for patterns in its symptoms, and finding that it is really two diseases (or something similar), we’d be interested to hear about that, since we can’t think of any examples where this approach has worked.
In the original potato diet study, we asked people to try to eat nothing but potatoes. This worked pretty well — people lost 10.6 lbs on average over just four weeks.
But we also told them, “perfect adherence isn’t necessary. If you can’t get potatoes, eat something else rather than go hungry, and pick up the potatoes again when you can.”
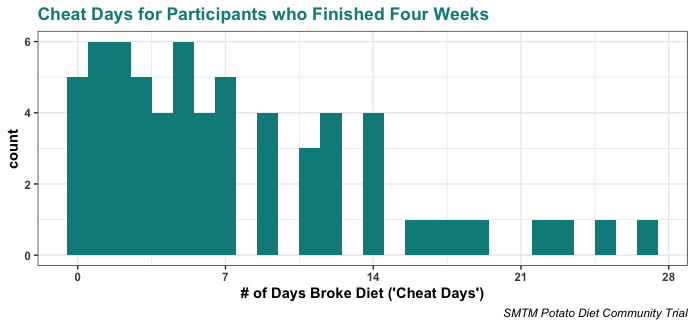
People took this to heart. We asked people to track how often they broke the diet, and almost everyone took at least one cheat day.
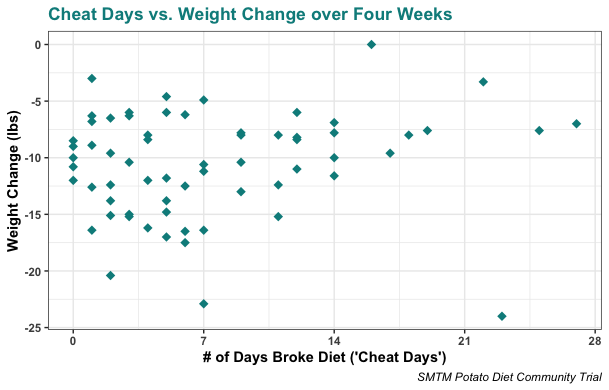
Five people said they stuck to the diet 100%, but everyone else said they broke the diet at least once. Most people cheated only a few times, but as you can see from this histogram, a substantial minority cheated more than half the time:
Taking these cheat days didn’t seem to matter much. Almost everyone lost weight, even if they cheated a lot:
In general, the more often people cheated, the less weight they lost. But even the people who cheated the most still lost around 5 lbs.
Realistically, our original potato diet study was really more like a 90% potato diet. People took quite a few cheat days, and it mostly didn’t seem to matter. Makes you wonder how low we can push that percent and still have it work — after all, the original weight loss effect was ginormous.
This is one reason why today we are announcing a 50% potato diet study. We’re looking for people to volunteer to get about 50% of their calories per day from potatoes for at least four weeks, and to share their data so we can do an analysis. You can sign up below.
Case Studies
The other reason we’re doing this study is a number of extremely interesting case studies.
Case Study: Joey No Floors Freshwater
The earliest case study comes from Joey “No Floors” Freshwater, who shared his story on twitter. He did a version of the potato diet consisting of “1-1.5lbs of potatoes a day when I could”. This comes out to about a 20% potato diet, and it turns out the 20% potato diet works quite well, at least for Joey.
Sadly Joey is no longer on twitter, but we do still have the screenshots:
Nicky Case Study: Nicky Case
The second case study comes from Nicky Case. Nicky participated in the original potato diet study and lost more than 10 lbs over four weeks, without much difficulty. This is kind of striking because Nicky was pretty lean to begin with.
After the potato diet ended, her weight slowly climbed back up. So 50 days after the end of the potato diet, she started a half-tato diet (“at least ONE meal per day is potato”). On the half-tato diet, she lost weight at about half the rate she did on the potato diet, and described it as “TRIVIALLY EASY to do”. Here’s the figure:
This is very encouraging. Nicky tried both the potato diet and the half-tato diet for more than 40 days each, and the direct comparison makes it pretty clear that the half-tato diet caused about half as much weight loss, at least for her.
M tried a version of the potato diet he calls “potatoes by default”. He describes this approach like so:
If I didn’t have anything better to eat, I’d eat potatoes. This meant that if I had plans for lunch or dinner, I would eat whatever it was I would’ve normally eaten ad libitum, and I tried actively to prevent the diet from materially interfering with my lifestyle (I drank alcohol socially as I normally would’ve, I participated in all the meals I normally would’ve participated in with friends, I tried arbitrary new dishes at restaurants, etc.). … In practice, “potatoes by default” meant I was eating potatoes for roughly 1/3 of my meals, mostly for lunch when I was working from home during the week or on weekends, since I usually had dinner plans of some kind.
This relatively potato-light approach caused surprisingly rapid weight loss. M describes it like so: “I think my main reaction to the data was that it was kind of insane? I was eating potatoes a third of the time and literally whatever else I wanted the rest of the time, and losing weight almost as quickly as the full potato diet.”
Here’s the figure. The chart on the right is just a zoomed-in version of the chart on the left, the vertical red line is when he began the potato diet, and the gray bars are when he was traveling and ate no potatoes:
The orange dots in this plot follow the daily averages for the full-tato diet we did. You can see that they are very similar to the blue dots, which are M’s data. When M says that he was losing weight almost as quickly as the full potato diet, he wasn’t joking. While the half-tato diet worked about 50% as well for Nicky, “potatoes by default” seemed to work much better than 50% for M.
You’ll also notice that M kept on “potatoes by default” for much longer than 30 days, and while the weight loss seems to slow a bit near the end, he keeps losing weight for basically the whole period covered in the plot. He loses more than 10% of his body weight over about three months! And he wasn’t even getting that many calories from potatoes — only like 30%!
Design
That’s why we are running a half-tato diet community trial. Let’s take a look at the design!
Half-Tato Diet Protocol
The half-tato diet is very flexible. As long as you are getting around 50% of your calories each day from potatoes, you’re on target.
Here are three ways of doing half-tato:
❖ True Half-Tato: Try to get 50% of your calories from potatoes each day, however you want.
❖ Potatoes-by-Default: This is M’s plan, and it worked well for him. Basically, if you don’t have any other plans for a meal, eat only potatoes (a little cooking oil and spices/hot sauce are ok, but nothing substantial). Otherwise, if you are seeing friends or going on a date or anything else, eat as you normally would. If you choose this plan, consider taking a close look at M’s email to us where he describes his protocol in more detail.
❖ Potato Meal: Have one meal a day be nothing but potatoes (with basic spices, etc.). For other meals, eat as normal. This is basically what Nicky Case tried for her half-tato diet. She describes it as “½ the weight-loss effect, but it was *much* easier than Full-Tato. Trivially easy, even.”
On the signup sheet (linked below), we will ask you to indicate which approach you are planning to follow. You don’t have to stick with the approach you choose, but it will be good to know which approaches are most popular, and if there happens to be a big difference between these approaches for some reason, maybe we’ll be able to pick up on it.
When you’re not eating potatoes, please eat as you normally would. The goal is to see how the diet works when you otherwise eat, exercise, and live as normal, so try not to change too much.
We do, however, have two small suggestions.
In the original potato diet study, we asked people to try to avoid dairy. But now we are not so worried about it. For the half-tato diet, please feel free to continue eating dairy if you want. We will just ask you to track the number of servings of dairy you eat each day on your data sheet. That way, on the off chance that dairy does make a huge difference, we may be able to detect it.
The second has to do with tomato products, especially ketchup. We reached out to the case studies we mentioned above, and most of them told us that they didn’t have ketchup with their potatoes, or didn’t have it very often, so “no ketchup” may be important for the half-tato diet to work. You may want to avoid tomato products and not have ketchup with your potatoes, but it’s really up to you.
Like with dairy, we will just ask you to track the number of servings of tomato products you eat each day on your data sheet. That way, if tomatoes stop the potato effect for some reason, we may be able to detect it.
To sum this up:
Get around 50% of your calories from potatoes each day, using whatever method (one potato-only meal a day, potatoes-by-default, etc.) you like.
Start with whole, raw potatoes when you can, consider cooking them in a way that keeps them as whole as possible.
Otherwise, eat as you normally would. Don’t consciously eat better, but also don’t consciously eat worse.
On the spreadsheet we share with you (below), track your weight, approximate percent potato for each day, your energy, mood, and the ease of the study, as described on the sheet.
Track servings of dairy just in case, don’t bother avoiding it if you don’t want to.
Track servings of tomato products, just so we can see if there’s a difference. Maybe consider avoiding them, especially if you’re not losing weight.
Track any bonus variables you’re willing/interested to track.
On the first day of half-tato, start eating potatoes as per the approach you chose above (e.g. potatoes-by-default). As long as you are feeling ok, keep trying to stick with it. The effect sometimes takes a couple days to become clear; there’s lots of variation between different people; you may lose a little weight one day and gain weight the next; don’t worry if the effect takes a little while to show up.
If you start feeling bad or weird, try one of these helpful hints:
Eating a potato (or something else). Hunger feels different on the potato diet and you may not realize that you are hungry. Yes, really.
Drinking water.
Eating a different kind of potato. Different varieties of potatoes may seem like they’re all pretty much the same, but they can really be quite different, and if you’re eating a lot of potatoes, these differences become much easier to notice. You will almost certainly want to eat more than one kind of potato.
Peeling your potatoes. Eating less peel / no peel seems to help some people with digestive and energy issues, especially after a few days on the diet.
Eating more salt. Potatoes are naturally low in sodium and you may not be getting enough. They’re also high in potassium, which can throw off your electrolyte balance if you don’t get enough sodium to match it.
If you try these things and still feel bad or weird, take a day or two off the half-tato diet and just mark down on your sheet that 0% of your food (or whatever) for those days was from potatoes.
If you start feeling really bad, or you otherwise can’t make the half-tato work for you, just stop the trial early. We don’t want anything bad to happen to you. Just send us an email to close out the trial as normal (see below).
Two-Week Baseline
In our previous community trials, we didn’t include a control group. This is because we expected the effect sizes to be ginormous. People don’t, generally speaking, spontaneously drop 10 lbs in four weeks, so it’s clear the weight loss on the potato diet is “real” without the need for a control group.
This worked less well for the potassium trial, but we wanted to get the biggest sample size we could for that study, and we weren’t sure how many signups we would get beforehand. We stand behind the idea that when you’re trying to estimate an effect size, it’s good to get as many people in the experimental condition as possible.
We’re still not going to include a control group, because we don’t think it would be very interesting to recruit half of you to sit around and do nothing for several weeks, and it wouldn’t teach us very much.
But we will do the next-best thing, and that’s to ask you to take a baseline of your weight change without the half-tato diet. For the first two weeks of the study, eat as you normally would, and track your weight over time. Then on the fifteenth day, start the half-tato protocol and get on to eating lots of potatoes. It’s simple.
This lets us use everyone as a control group for themselves, sort of like a crossover design. While this design wouldn’t work for everything, we think it works pretty well for the half-tato diet.
Variable-Span Signup
We’d like you to try the half-tato diet for at least four weeks. With the two-week baseline, this is a total commitment of six weeks.
But if you’re willing to go further, we would be really interested to have that data. So for the half-tato diet community trial, we are opening things up and letting people enroll for however long they want.
Credit where credit is due, this part of the design was Nicky Case’s idea. She describes it as a “hey this trial runs for however long you want, and we’ll just report data every month for whoever hasn’t dropped out yet” design, and we think it makes a lot of sense.
This is a bit like what we did with the potassium trial — we asked people to keep going to 60 days if they were willing, some did, and we reported on their data in a second analysis post. We want to do the same thing in this study, except that we’d like to ask you to sign up for longer spans up front, if you’re willing.
We won’t hold you to this. It’s not a commitment. We’d just like to know up front how long you’re planning to sign up for. If you can’t make it that long, that’s fine. Just tell us how long you’re thinking you might try.
(Obviously you can also keep going for longer if you want, don’t let us stop you.)
For example, you can sign up for:
2-week baseline + 4-week half-tato
2-week baseline + 8-week half-tato
2-week baseline + 12-week half-tato
And so on and so forth, all the way up to 2-week baseline + 68-week half-tato. We will take snapshots of the data at relevant intervals and analyze the data up to that point.
Sure, “report every month on whoever hasn’t dropped out yet” has a selection bias. The people who sign up for 52 weeks will not be your average ordinary citizens. In fact, they will be paragons, heroes. But that doesn’t concern us. We still want to see those data.
And if you sign up for 52 weeks but it turns out no one can actually be bothered to do half-tato that long, that’s still useful data. Just think about it. 😉
Sign Up
Ok researchers, time to sign up.
The only prerequisites for signing up are:
You must be 18 or older;
In generally good health, and specifically with no kidney problems;
Willing to do a two-week period of baseline measurements;
Willing to get about 50% of your calories every day from potatoes, as described above, for at least four weeks, and;
Willing to share your data with us.
As usual, you can sign up to lose weight, lower your blood pressure, get more energy, or see one of the other potential effects. But you can also sign up to help advance the state of medical science. This study will tell us something about nutrition, weight loss, and obesity. If the half-tato diet works for most people, it will give us a practical weight-loss intervention that’s much easier than the 100% potato diet.
And beyond that, running a study like this through volunteers on the internet is a small step towards making science faster, smarter, and more democratic. Imagine a future where every time we’re like, “why is no one doing this?”, every time we’re like, “dietary scientists, what the hell?”, we get together and WE do it, and we get an answer. And if we get a half-answer, we iterate on the design and get closer and closer every time.
That seems like a future worth dreaming of. If you sign up, you get us closer to that future. We hope that this is only the beginning of what will be a century full of community-run scientific trials on the internet. Maybe by 2030, the redditors will have found a way to triple your lifespan. But for now we are doing potato.
Eating this much potato may sound a little daunting, but people who have tried it say that it is much easier than they expected, and delicious to boot. Here’s our suggestion: If you are at all interested in trying the half-tato diet, go ahead and sign up and start collecting your data. Collect your baseline measurements for two weeks, then try the first day or two of half-tato and see how it feels. If you hate it and have to stop, we would still love to have that data.
If at any point you get sick or begin having side-effects, stop the diet immediately. We can still use your data up to that point, and we don’t want anything to happen to you.
We are mostly interested in weight loss effects for people who are overweight (BMI 25+) or obese (BMI 30+), but if you are “normal weight” (BMI 20-25) you can also sign up. The original full-tato diet caused weight loss in people of normal weight, and it would be interesting to see if the same thing happens for the half-tato.
And for everyone, please consult with your doctor before trying this or any other weight loss regimen.
If you were part of the original SMTM Potato Diet Community Trial, or the SMTM Low-Dose Potassium Community Trial, please feel free to sign up for this study as well! We know that most people who were part of the Potato Diet Community Trial have returned to their baseline weight in the last 6 months, so the original results shouldn’t interfere. And it will be very interesting to compare your weight loss on the half-tato diet to your weight loss on the full-tato diet. Since we can make direct within-person comparisons, this will give us a much better sense of if the half-tato diet works half as well (or better; or worse) as the full-tato diet.
Anyways, to sign up:
Fill out this google form, where you give us your basic demographics and contact info. You will assign yourself a subject number, which will keep your data anonymous in the future.
We will clone a version of this google sheet and share the clone with you. This will be your personal spreadsheet for recording your data over the course of the diet.
On the first day, weigh yourself in the morning. If you’re a “morning pooper”, measure yourself “after your first void”; if not, don’t worry about it. We don’t care if you wear pajamas or whatever, just keep it consistent. Note down your weight and the other measures (mood, energy, etc.) on the google sheet.
For the first two weeks, eat as normal and continue to track your weight and other variables to provide the baseline. Then when the two weeks of baseline are complete (clearly marked on the data sheet), start eating about 50% potatoes, and continue with the half-tato diet for however long you signed up for (4 weeks or longer).
We prefer that you try to get around 50% of your calories from potatoes for at least four weeks. But imperfect adherence is ok. If you only get 30% of your calories from potatoes one day, or you have to skip a day entirely, that’s all right. Just note it down on your sheet. We’re interested in how the diet works for normal people at home, with all the complications that entails.
When you reach the end of the diet (whether you’re ending the diet early, reaching the span you signed up for, or going beyond it), send us an email with the subject line “[SUBJECT ID] Half-Tato Diet Complete”. This will give us a sense of how the study is proceeding in general and is your opportunity to tell us all about how the study went for you. Please tell us any information that doesn’t easily fit into the spreadsheet — how you felt, what kind of potatoes you used, how you prepared them, before and after pictures (if you want), advice to other people trying this, etc. There’s a chance that the half-tato approach will work for some people and not for others, and if that happens, we’ll dig into these accounts to see if we can figure out why.
Remember that it is ok to end the study early if you need to, for example if you get sick, or if you decide that 12 weeks or whatever is too long of a commitment. It’s also fine to reach 12 weeks and keep going if you’re having a good time. Just make your intentions clear in the comments on your data sheet and send us an email whenever you decide to finish, we’d love to hear from you.
Assuming we get 20 or so people, we will write up our results and publish them on the blog. We would really like to get a couple hundred people, though, since at that point it becomes possible to do more complex statistical analyses. So if you think this is an interesting idea, please tell your friends!
This post is an interview with some guy, writing under the name Exfatloss, who has been conducting a weight loss self-experiment and recently put out a blog post about the results so far.
Exfatloss has tried a lot of different weight loss techniques, including the potato diet, but nothing seemed to work over the long term. Until now, that is. He has invented a diet he calls “ex150” that has caused a surprising amount of weight loss, and which seems to be quite reliable — at least for him.
This interview is lightly edited for clarity, and to make Exfatloss “sound smart and funny” per his request.
Exfatloss: Hey SMTM, I finally wrote up a summary on my crazy diet experiment, now that I’ve lost just over 43lbs in 5 months. It has a weight graph that I hope you find enlightening.
Feedback from an experimental/author/publication/science/whatever perspective highly appreciated!
SMTM: This is very exciting, and it makes us want to drink some heavy cream right away, yum. Several questions:
ex150
SMTM: For starters let us make sure we understand the ex150 diet as you describe it. It involves:
Eating just one meal per day, of:
~150 g meat, usually as
ground beef chuck (80% lean / 20% fat) or
ribeye steak
~60 g green vegetables, usually as
microwaved frozen vegetables “(okra, spinach, green beans, fajita mix)”
~80 g pasta sauce, usually as
“the sauce is low-everything and mostly water (e.g. most store brand tomato/alfredo pasta sauce)”
I.e. either red or white sauce
As much butter as you want to cook these things in. (“usually about 15g”)
None of these things measured or weighed precisely, i.e. the diet seems quite flexible. “I don’t think the exact number matters much.”
Exfatloss: Initially I just cut a 1lb thing of ground beef into thirds. It’s pretty much exactly 150g that way. I’d say it doesn’t matter much if you do 130g or 170g. That’s what I mean by “exact numbers don’t matter much.” If lack of a kitchen scale is holding you back, don’t worry about it, eyeballing it worked fine for me. Now if you were to eyeball double the amount of meat… I dunno. I’d consider that more “ex300” than “inexact numbers.”
tl;dr, just buy 1lb of meat and cut it into thirds.
SMTM:
Otherwise eating no meals but:
butter and whipped cream, as much as you want, as snacks/desserts
Sometimes with instant coffee powder for flavor or tomato sauce to cut the fat taste
Quite a lot of it, “I go through a lot of cartons of heavy cream, maybe one every 2-4 days.” How big of a carton? 16 oz?
As a result, most calories come from cream.
No-calorie foods like coffee are also ok, including coffee with arbitrary amounts of cream, and including going to Starbucks.
Exfatloss: The heavy cream comes in 32oz. I have 3 of those in my fridge right now. I think it’s about one 32oz carton every other day I go through. I put instant coffee powder in the whipped cream most days for flavor.
SMTM: Also you are currently in the USA right?
Exfatloss: Yes, and have been for this entire weight loss period so far.
SMTM: As we understand the intent behind the design, the butter and whipped cream are there to make it high-fat, the 150 g meat is there to make it a low-but-nonzero protein diet, and the vegetables are there to give some minimum amount of fiber. Does that seem right?
Exfatloss: Vegetables for flavor/texture and minimal fiber, yes.
Pure ground beef tastes like shit. Trust me, I’ve tried it.
Butter/cream are there to provide calories that are not protein/lithium/whatever the factor is. They’re a known-not-fattening source of calories that also happens to cause no bloating and that I deal with super well.
SMTM: Butter and cream are “a known-not-fattening source of calories that also happens to cause no bloating”? Our sense is that most people would assume that butter and cream are fattening and might cause bloating, so the fact that you seem so confident is surprising. Known to whom, how? It’s news to us!
Exfatloss: Well, known to me, at this point 😉 Through trial and error. There are a bunch of people with theories why (low protein, low PUFA, low UFA).. but honestly I have no clue if any of them are right. I just know I lost a bunch of weight eating mostly heavy cream.
I think it’s an important factor of any sustainable diet that you are NOT in a caloric deficit, or it won’t work (Caloric deficit symptoms -> “willpower breakdown” -> quit diet).
SMTM: This also really stands out! It does seem to fit with what we saw on the potato diet. How did you come to this conclusion?
Exfatloss: Decades of experience? Pretty much any time you restrict your intake or increase your expenditure, you can expect to keep it up for 1-3 weeks or maaaybe if you’re really hardcore a bit longer, and then it stops working and you lose “willpower.” That seems like THE ultimate diet experience of everybody who’s ever tried to lose weight. I write about this in my latest post.
Also when people say “deficit” they are super vague and conflate things and that’s why it’s both necessary and impossible to run a deficit to lose weight. Planning on writing about this at one point.
SMTM: What is the pasta sauce there for? You say, “mostly water”, is that also part of the design?
Exfatloss: Flavor and to soak up the fat 🙂 It tastes significantly better with the sauce. Maybe that’s just me. This whole meal is my previous go-to meal for over 3 years, just scaled down. I used to eat 1lb of that stuff per day, now it’s ~170g and I added the cream to make up for the calories.
SMTM: It may not matter, but we’re curious, what method do you use to test whether you’re in ketosis? If you tracked your ketones data it might be interesting to graph or publish it as well.
Exfatloss: Currently using a ketone blood meter (finger prick style). I will say a lot of carnivore peeps are calling my “zero fiber != ketosis” statement BS and I’ve updated that section of the blog post to clarify.
Since ketone blood strips are expensive and annoying I haven’t tracked those in years, since first starting keto 7 years ago. So unfortunately no data to show 😦
Would be cool if CGMs could track more than just blood glucose! I would love to have years worth of ketone levels. Good news is that the next-gen Libre Freestyle CGM will have this! Very excited.
Palatability and Variability
SMTM: In your post you talk a bit about hypotheses, including this one:
Palatability/brain hack: there is a lot of science out there around the brain’s ways of dealing with food, food reward, and metabolism. Stephan Guyenet’s The Hungry Brain is maybe the best summary, I think. I’ll admit I haven’t read the book, but I listened to a few podcasts where he talks about the ideas, and I think the ex150 diet fits his hypothesis. The idea is that hyper-palatable food that is very energy-rich causes us to overeat in terms of energy. The ex150 diet has 1 hyper-palatable meal every day, but it is very small. The remaining calories come from a bland mono-food that’s hard to overeat (heavy cream). Maybe this tricks the brain into not overeating the cream, yet never feeling more than 24h away from a hyper-palatable meal to release lots of dopamine or other happy food reward signals? I think that even if this might not be the main causal factor, it sure helps make the diet sustainable. I’m never more than 24h away from the most delicious meal I could imagine, and I can eat unrestricted amounts of “dessert” (=whipped cream w/ instant coffee powder).
This mostly seems like evidence against the palatability hypothesis to us, though it might be interesting to ask Guyenet what he thinks. But to us it seems like you are eating delicious foods and getting a lot of food reward. If as much heavy cream and butter as you want plus “the most delicious meal I could imagine” counts as “low palatability”, then the term is so meaningless that it should be tossed out.
Exfatloss: I do personally think that “palatability” (and “satiety”) are meaningless the way they’re often used, even by Guyenet. I heard him on a podcast where he basically said (paraphrasing) “Science has found that humans tend to be caused by their brain to overeat foods that have high palatability.” Wait, isn’t that the definition of palatability? Very roundabout way of saying “Food that tastes good tastes good.” 😀
SMTM: Yeah that has always seemed kind of circular to us.
Exfatloss: I’ve @mentioned Guyenet on Twitter, but he didn’t reply (maybe cause I’m a nobody lol). Maybe I’ll ask him again when I have street cred lol. I do think he’s a good representative/explainer of “The Science” on this because he’s got a good grasp of various ideas out there and has been in full-contact debates with Taubes etc. and was able to hold his own. I respect him. I sometimes feel like citizen-scientism is bordering on anti-science and someone knee-deep in science like him is able to check that tendency. That said, in a fight, my money is on Taubes.
SMTM: We like Guyenet and he’s interacted with us a tiny bit, maybe we can help get his attention. We understand that he’s reluctant to engage with weird randos on the internet but we’d be curious to see what he thinks of this.
Exfatloss: Regarding the dichotomy here: I think the meat/vegetables/sauce meal has near infinite palatability, I’ve literally eaten a pound of this before scaling it down for ex150. So if this diet was “eat as many of these tiny meals a day as you want” I’d eat 15 of them. But I can only have 1. The cream/butter on the other hand has extremely low “palatability” in the sense that it’s very hard to overeat.
How do you know you’ve had too much cream? You’ll fricking know. It comes from one second to the next, where the thought of another sip almost makes you gag. Total on-off switch for me, whereas I can literally eat carbs until I puke and not be satiated (ask me how I know. College, man!)
So if “palatability” means something like “able to overeat” then cream is not it, because it’s very self-limiting. Potatoes and dry chicken breast are also very self-limiting, but they’re in fact so limiting that I got into a massive deficit, got caloric deficit symptoms, and had to quit the diet (plus all the fiber made me feel bloated and gross).
SMTM: Your results look a little more like the variability hypothesis, though. We interpret this as a version of (or closely related to) the palatability hypothesis, where the problem is not tasty foods per se, but eating a variety of foods that are tasty in different ways. We think this theory is poorly-supported but ex150 is definitely a low-variety diet, mostly consisting of the same 5 or so foods eaten every day, however delicious they might be.
It’s clear that ex150 is a low-variety diet, close to a mono diet. But it also seems like variety or mono-ness aren’t the active ingredients here because you did other low-variety and/or mono diets and they didn’t work for you at all. If low-variety or mono diets worked for you, then you would have lost weight on the other low-variety/mono diets you tried — on the carnivore diet, on the “eating only at In’n’out burger” diet, and on the potato diet.
Exfatloss: Yea I do think there’s something to “variety -> overeating.” I do think mono-foods “work” in being self-limiting. My hypothesis here is basically that ex150 manages to hit the goldilocks zone – 1 hyper-palatable meal per day and the rest is a self-limiting mono-food, but it’s not so mono that you get into a massive deficit that makes the diet unsustainable (like potatoes did for me).
On my first week of Potato I was doing only boiled potatoes sans everything, and I couldn’t get down more than 600kcal per day. I’d force myself to go to the fridge, grab a boiled potato, take a bite. It’s not even that the bit tasted bad – but after 1 bite, I was almost gagging. I just couldn’t take a second bite.
So clearly too self-limiting to be sustainable. 200ml of heavy cream has almost 700kcal just on its own and you don’t have to boil it, doesn’t come with all the bloating fiber, digests super easily. Plus you can put instant coffee in it 🙂
SMTM: This isn’t our sense of how the potato diet works in general, since it seems like the tato makes you LESS INTERESTED in other foods.
This seems especially clear in people who have tried half-tato diets. They let themselves eat other foods, but eating a big chunk of potatoes on a regular basis seems to lower your appetite for everything else. For example see M’s experience on the half-tato diet. He says, “maybe two or three weeks in, for the first time in a really long time, I did not have the urge to finish off leftover food at dinner.” Or Joey No Floors Freshwater, who said, “The difference is now I get full and stop eating. I leave food on the plate, which is new for me. I leave texmex on the plate y’all. Its wild.” So the potato diet doesn’t seem to work on just the self-limiting aspects of potatoes because people are less interested in eating other foods too.
That might be one more reason to do a larger half-tato diet study, to see if this generalizes.
Exfatloss: Hm, that sure wasn’t my experience. For me, it was just an inefficient fast plus the worst bloat in years.
I only did full-tater, maybe half-tater would’ve worked better for me? Not sure why it would work so awesome for some and so badly for me.
One theory I have for that is the goldilocks satiety idea. If you eat a mono food and it’s not satiating enough, you’ll overeat and gain weight. If it’s too satiating, you won’t be able to eat enough to meet energy expenditure and you’ll begin getting caloric deprivation symptoms and will eventually land in caloric bankruptcy (see my post).
Not sure why exactly potatoes don’t hit goldilocks zone for me but do for others. Maybe I have a higher energy expenditure or do worse on potatoes?
Re-reading the section of those people who had potato-success, I do think there’s something to “fix satiety.” Maybe the common thread is that these diets somehow fix satiety in people whose satiety signals are broken.
Of course that just moves the question to “how did the satiety signals break and what fixes them?”
SMTM: To us this looks like evidence against both palatability and variability in your case, and some evidence against them in general, especially if it turns out that ex150 works for other people.
Exfatloss: As those hypotheses are commonly understood, yea. But maybe the Goldilocks Palatability thing? 🤷
I.e. it’s not that “lowest palatability/variety” is optimal, but “modest palatability/variety?”
SMTM: Some other theoretical explanations do come to mind. You’re probably eating close to zero calories from seed oils, so while we don’t find seed oils to be a very plausible theory of obesity, we want to at least note that this result is very consistent with that theory.
Exfatloss: Yea, I’ve actually kind of added that as a new hypothesis. I found this insane s/saturatedfat subreddit after posting my article. People there were like “Duh, of COURSE you would lose tons of fat by eating saturated fat!” There’s this guy Fire in a Bottle (twitter/youtube) who has this whole theory how modern meat (even beef) is full of TCCD (I forget what it stands for but it’s BAD cause CHEMICALS) and PUFAs etc. and that’s what’s making us fat.
I will say I did Paleo for 3+ years before Keto, and Keto for 7 years before this, so it’s not like I was chugging seed oils. But I was eating TONS of US commercial grown beef. So if it’s in that..
It would be cool to design experiments to kind of disentangle the various hypotheses, although I’m not sure exactly how. I suppose a month of 2lbs/day of grass-fed beef? 🤷 Maybe ask the gurus who recommend those theories to design an experiment? They’d know.
SMTM: We also notice that “lots of pure fat” does sound kind of like the Shangri-La Diet, so there might be some connection there. A chemical engineer we work with has repeatedly emphasized that while lithium probably accumulates in many foods, it shouldn’t end up in oils because it’s not fat-soluble. Maybe this is connected to why high-fat diets sometimes work? This isn’t limited to lithium, it’s just generally a note that if obesity is caused by a contaminant, there’s some reason to think that the contaminant doesn’t accumulate in fats.
Exfatloss: Interesting, yea. I remember reading about Shangri La years ago. It does seem very similar. Question is why, I guess: is it “appetite suppression” and what does that even mean – ensuring energy balance is met or some psychological thing?
Have you sent a bunch of meat/milk/cream/potatoes to the lithium lab yet? That would shine some light on it, I imagine.
SMTM: We’re working on it! 😉
Potato Diet
SMTM: The fact that you didn’t lose any weight on the potato diet and “HATED how bland it was” seems really interesting, especially given that most people on the potato diet said they loved it and many talked about how delicious they found the potatoes, even after 30 days. And for the most part, obese participants had the most success on the potato diet, so it’s interesting that you found it boring.
It kind of suggests there might be at least two kinds of obesity, one that responds to the potato diet and one that responds to ex150. If something like that were the case, it would be pretty easy to demonstrate experimentally.
Exfatloss: I’ve long suspected that obesity is a “slightly complicated problem.” My analogy is a broken down car.
You drive by a car broken down by the side of the road.
You say: “Have you tried putting gas in the tank?”
“Yes, still doesn’t drive.” says the guy
“I’m pretty sure putting gas in cars works, my friend broke down once and he put gas in the tank and then it worked again.”
“Doesn’t work for me,” says the guy in the car.
“I think you’re just not putting enough gas in the tank,” say you.
That’s basically the state of our discourse on obesity, when even much simpler things like cars can break down for a handful of reasons. Maybe spark plugs. Flat tire. Crankshaft. Hell, I’ve had a cylinder blow up on me because the timing belt skipped a beat and one of the cylinders fired out of order.
If there were 4 causes of obesity and 4 different diets to fix them, we would currently conclude that there is no solution and we don’t know and nothing works better than anything else, because we insist on averaging everything out.
On average, putting gas in broken down cars’ tanks doesn’t work. But sometimes it does. When lack of gas is the problem.
SMTM: Yes! We’ve been working on a post about this. People spend a lot of time saying obesity is a disease when clearly it is a symptom that can be caused by all kinds of things. So while there could be just one epidemic, there could equally be several.
There could even be several epidemics for just one reason. If you roll a bunch of cars over a cliff, many of them will break when they hit the bottom and won’t be able to start. But they might all end up broken in different ways, even if the ultimate cause is “was rolled off of a cliff”.
Exfatloss: Yea “disease” has always seemed wrong to me. I get that people want to take the moral stigma out of it, but “disease” sounds like your immune system will clear it out after 2 weeks or it’s a viral infection or something.
If anything, I’d call it a “condition.”
SMTM: Your experience actually seems like some evidence against the contamination hypothesis and in favor of some kind of deficiency hypothesis. Let’s say that obesity is caused by a deficiency in either X or Y. Potatoes contain X and heavy cream contains Y. If you are X-deficient but have good Y levels, then the potato diet will cure your obesity but cream will taste gross because your body is trying to avoid overloading on Y. If you are Y-deficient but have good X levels, then ex150 will cure your obesity but potatoes will taste gross because your body is trying to avoid overloading on X.
Exfatloss: I don’t know if I agree, it could easily be consistent with contamination. Maybe potatoes and fats are both very low in contaminants, but some people do super well on fiber and starch whereas others do better on fat. I’m sure people with dairy intolerance will hate my diet, but I used to chug a quart of milk for breakfast as a kid and I can dairy all day. Others apparently love potatoes all day. Personally I do best on “close to zero but not quite zero” fiber.
I think the “feels good on X/Y diet” and “contamination” theories can exist side by side and explain this.
SMTM: Would you be at all interested in running an ex150 community trial, maybe recruiting specifically from people who also found the potato diet bland/difficult? You could start by just getting a couple of other people to try it as case studies, since there’s a rather blurry line between “2-3 case studies” and “community trial of 10-20 people”. If the effect is as strong for other people as it is for you, you wouldn’t need a very big sample size to produce convincing results.
Exfatloss: Yea, definitely. In fact I’m trying to recruit some of my friends 🙂 One insisted on switching to the diet at the same time as doing CrossFit for the first time, because apparently isolating variables is for losers…
If you pointed a couple people my way I’d be happy to set up some kind of study. People can contact me on twitter or the blog, or can email me at hello@exfatloss.com
SMTM: Absolutely! People will see it in the blog post and we’ll share about it on twitter, we’ll encourage people to email you there.
Exfatloss: Sounds good!
If it’s just a handful of people I think I’d be more comfortable managing it. I’m not sure I’d be up for hundreds of people like you had on Potato because I’ve never done that type of thing before. That seems to require infrastructure.
SMTM: Yes, and it’s good to start with more case studies before scaling it up to dozens of people. Better to make sure it generalizes and we can re-create it so we don’t waste everyone’s time.
Exfatloss: Yea for sure. Maybe I’m just somehow a crazy sat fat outlier who can’t deal with potatoes 🙂
Boundary Conditions
SMTM: You mention,
For example, could you make the diet work eating only at common fast food restaurants? Using only prepared deli meats? What about cheese? Is it really just about the amount of protein, or does it matter what kind of protein? Eggs?
Does the diet even need to be ketogenic? What happens when you reach a healthy weight, can you back off the diet? Do you cycle it? Is there a maintenance version?
These seem like the most important questions to us. If you switched to 150g eggs + different vegetables + as much olive oil as you want, would it persist? What about other formulations?
What if you stick with the original formulation but slowly add rice until you are no longer in ketosis? You wouldn’t necessarily need to go out of ketosis if you could show a correlation between the rate of weight loss and your ketone levels (though obviously dropping out of ketosis without it affecting the weight loss would be most convincing).
Exfatloss: I’m actually currently on day 5 of ex150deli, which substitutes supermarket deli meat cuts (salami, turkey breast, roast beef..) for the ground beef. I kept the vegetables/sauce the same for science’s sake and let me tell you, they do NOT go well together with sliced deli meats lol. [SMTM note: since finished with success, see here]
Agreed that this would be awesome. It seems there’s gotta be a whole lot of alpha out there in fat loss, and we’re probably nowhere near the efficient frontier. So we should explore the boundaries. What do we actually have to give up to be successful? Why give up more.
SMTM: We also noticed that you say,
What piqued my interest though was that the super-low-protein carnivore diet, while it still kicked me out of ketosis, made me rapidly lose weight, about 10lbs in the 12 days until I ended the experiment early (because I was out of ketosis already, proving the hypothesis).
This story suggests that such a thing is possible.
Exfatloss: See my 2/17/2023 update on the post on the fiber/ketosis issue, several carnivore people claim I’m wrong on this and I concede it’s possible.
SMTM: It also seems like this could just be a cream-maximalist diet, right? Do you know about how many calories you’re getting per day, and how many of them are from cream? Seems like it’s over 50% right?
Exfatloss: 50%? Ha. It’s 85% before I add the cream in the coffee 🙂 I have a macro estimation in this blog post.
SMTM: There would be a darkly comic element if obesity was cured by high doses of cream, but it would also make some sense. What is the one treatment for obesity that no one would ever think to try? “Drink as much heavy cream as you can stand, every day.” We’re confident that most people would never try this (ok maybe some people would on keto), so it would make sense if everyone missed it…
Exfatloss: Ha you should see the r/saturatedfat people.. as I understand it, the claim is literally that eating saturated fat will increase your metabolic rate by insane levels and thus create a massive bottom-up deficit.
SMTM: In general, is there a principle of “if you’ve been looking for a long time and tried everything you can think of and nothing works, the real answer must be something that seems really stupid”? Reminds us of Sherlock Holmes’ “when you have eliminated the impossible, whatever remains, however improbable, must be the truth.”
Exfatloss: I will confess to having read a lot of Sherlock Holmes.
SMTM: Us too!
Superstition and ABA
SMTM: Generally we are concerned about the “superstition” element of self-experiments. If spontaneous remission is a possibility, and you try a long enough list of things, you might randomly spontaneously remiss and it would look like the thing you were trying at the time is the cause:
Let’s say that Mary develops chronic fatigue syndrome (CFS). She is proactive and wants to solve the problem, so she comes up with a plan of 26 different treatments, which we’ll call A, B, C, D, and so on. Maybe A is “cut out dairy”, B is “walk 20 minutes every day”, etc. but the specific plans don’t really matter. She starts implementing each plan for two weeks, first plan A, then plan B, etc.
But the cadmium is slowly being cleared from her system by natural means at the same time as she works her way through the 26 treatments. What happens is this: Mary reaches treatment L (“take omega-3 supplements”) just as the cadmium in her system drops below critical levels, and Mary is immediately “cured”.
Since her symptoms stop almost immediately after starting treatment L, Mary assumes that the omega-3 supplements are what cured her, and continues taking them indefinitely.
This is basically what happened when you moved back to the US from China.
So we REALLY like how you took a 14-day break from ex150 right in the middle of your self-experiment. If you were randomly losing weight for some other reason, then you should have kept on losing weight during this break. The fact that you gained weight back, and that it closely corresponds to the break (modulo pemmican), seems like strong evidence that, as you say, “it wasn’t some other random factor in the environment causing the fat loss.”
We see the same thing in a smaller way in two other short breaks you take.
This looks a lot like an ABA design, or since you have four experimental periods, an ABABABAB design.
Usually we would say that ABA-type designs don’t really provide enough evidence to draw clear conclusions. Even with an ABABABAB, that’s still only a sample size of 8 intervals. But in this case, the effect seems so distinct and so the effect size so huge we’re not sure. What do you think?
Exfatloss: Definitely agreed that it doesn’t prove “what did it” or even anything.
But it disproved a bunch of really likely environmental factors like a) city (walkability? air quality?) b) weather/temperature c) drinking water d) cancer haha.
I think it’s a really easy and pretty good thing to do. If you really know why the light turns on and off, you shouldn’t be afraid to hit the switch a couple of times and see if it works as you thought. That’s kind of the least you can do. If you never turn the light off because you’re afraid it won’t come on again, does that really sound like you understand why it’s on in the first place?
Set Point
SMTM: In your Q&A section you give this exchange:
Q: You’re just going for walks now.
A: No, fat loss started 2 months before that and the rate hasn’t changed. But yes, I feel so energetic many days on this diet that I started spontaneously wanting to go outside and take long walks. One time I even fell into a light jog! In my experience this is a result of effective fat loss, having “unlocked” the key to utilizing my body fat, not the cause of fat loss. 1,150kcal/day (0.3lb of body fat) would be a long walk to take every day.
This is interesting to us because it suggests your set point is falling faster than your weight is. Compare this experience to how you mentioned that running as exercise just makes you hungrier to compensate for the extra calories you burn. So that suggests that something about this diet changes your set point very quickly, which seems interesting.
Exfatloss: I kind of believe that we’re thinking about “set points” slightly wrong. This is inspired by my understanding of circadian rhythms.
All humans have a “genetically predetermined circadian rhythm.” But it’s not that somewhere in your genes it says “8am EST” or anything. The best analogy I’ve read is that what’s basically encoded is a spring weight. Imagine your circadian clock is powered by a spring, and sunshine pushes down on the spring. Different people have different spring weights. Most people’s weight is such that if they get even a little bit of sunlight during a normal day, their spring is fully compressed and ready to go again. Some people have a very stiff spring, and they need enormous amounts of sun exposure to get it compressed during one day.
If you move even normal people to the north pole or something, even their springs will never compress (in the constant dark) or always be overcompressed (in the constant sunlight). If you put people in a cave, the spring mechanism just completely stops working.
My point being, what if it’s not that we have a “set point” that says “He shall be 210lbs” but instead, the rate of how “calories in” is split up? Similar to the P ratio. This ratio could be influenced by various factors like macro composition, chemicals in the food, sunlight, sleep quality.. some people have a ratio in such a way that pretty much no matter what they do, the calories they eat will be sent to the furnace. Other people will have ratios that require them to take super extreme measures to prevent gaining fat. If you put healthy people on a PUFA-sugar-juice diet and sleep deprive them and feed them tons of lithium, even they will probably gain fat.
For example, maybe I’m just an insulin hyper-responder, and what normal people consider “normal” amounts of carbs or protein makes me obese. And suddenly my ratio has swung from one end of the scale (->90% of calories in go to fat) to the other (->90% calories are sent to the furnace and you will fricking go for a walk every day even in freezing rain just cause you can’t stand sitting still).
Maybe it’s not that this ratio per se is encoded. Point is it could easily be encoded as a flow rate, not as an absolute “set point == 210lbs” value. And you just reach a different equilibrium with your current environment depending on the flow rate/spring rate. Just as you’ll reach a certain “waking set point” in the winter, and a different one in the summer, depending on factors like sun exposure.
SMTM: This is a good argument, but the difference between circadian rhythm and metabolic set point is that while the body doesn’t have access to a direct measure of time (it uses external cues like sunlight), it does have access to internal metrics about obesity. This seems to involve signals like leptin, literal compressive weight on your bones, blood sugar, stomach fullness, etc.
Exfatloss: But those metrics aren’t an objective, comprehensive obesity score like body fat %. It’s different chemical signals. Those signaling pathways can be disrupted or conflated or confused.
In a computer analogy, there isn’t one program in your body that can read the total fat storage value and set the heater/AC accordingly. It’s a bunch of distributed systems sending each other messages in various ways. If something goes wrong with some of the packages, unspecified behavior can set in. The TCP port could be blocked. The pipe could be broken. Your packages might get misrouted by a rogue/broken system in the middle. There might be backpressure in the signaling system that changes the frequency/density of the packages arriving.
Might also be personal. For example, my sensitivity to physical stomach fullness is practically zero. I always assumed that people meant this figuratively. I have literally eaten until I was painfully full and felt zero satiation. I wanted to continue, I just couldn’t, from the pain.
Pro-tip: never go to an all-you-can eat pizza place.
The potato diet wasn’t quite that bad, but it was also really bad.
On the other hand, the whipped cream satiety hits me like a cement truck. One bite fine, second bite good, third bite NO WAY I’M FULL. (These are the last 3 bites, not the first 3 bites, of a whipped heavy cream meal.)
SMTM: How about the hairpin turns when you try going off the diet and back on again? Whatever this diet is doing, your weight seems really responsive! That’s weird, but it kind of matches the results on the potato diet, which also seems to cause abrupt changes in most people’s weight.
Exfatloss: A lot of the hairpin is water retention. I’ve seen as much as +6lbs the day (!) after ending my second ex150 month, and -4lbs after the first day of pemmican.
One confounder with potato for me is actually that I was pretty low-fiber before it, because I hate fiber. So I went from a low-fiber to an all-fiber diet, which would jack up my water retention. So given the above numbers, even if I lost 6lbs on potato, the very first day of increased water retention could negate it.
Btw these water retention effects are plateau effects, which was my criticism of your recent potassium study. But if you do switchbacks, it creates these insane hairpin turns.
I basically disregard the first, really steep weight loss when I go on the diet. Usually it takes at most 5 days to finish the plateau effect and for the “real” fat loss rate to show.
Metascience
SMTM: We agree that the real point is the meta-framework of experiments, so we’re really interested to hear more about these other things you tried that you list near the beginning of your post (cold showers, no online news, carnivore diet), what can you tell us about those?
To emphasize: the real point is the meta-framework of experiments. Formulate a hypothesis, design a 30-day experiment, test it. I’ve probably done dozens of these over the years.
Here are some examples from the last few years:
30 days of cold showers
90 days of no online news (I thought stress might contribute)
90 days of the carnivore diet
30 days of eating only at In’n’out burger
Doing Starting Strength, a beginner’s powerlifting program
Doing Simple & Sinister, a kettlebell training program
30 days of drinking only distilled water (including for coffee)
Eating only pemmican, a raw meat paste invented by Native Americans
Exfatloss: Ha I’m planning to eventually write a longer post where I detail some of these experiences. [SMTM note: this post has since been written, see here]
Some highlights: cold showers did nothing. No online news (suggested by a friend) showed me that I consume news as entertainment, but that I just replace it with movies/video games when I stop consuming the news. Carnivore diet was super bland and boring (YES steak gets boring!) and I didn’t lose any weight. In’n’out was the best, I love that place! My first low-protein trial was entirely done at In’n’out, as was the low-fiber one. Starting Strength made me fatter. Pemmican was even more unpalatable than potatoes lol, I chewed every bite for 2 minutes. It just tastes like I imagine cow manure tastes like. Ugh. Sad because I really wanted to like it.
SMTM: A lot of science criticism seems really facile. In particular, it seems like lots of people don’t understand measurement, they think that measuring things is both objective and easy. It makes us wonder if these people have just never tried to measure anything for themselves so they don’t realize what is involved (compare: Reality has a surprising amount of detail). So our sense is that trying a lot of failed diets is part of what has made you a careful experimenter. What was your experience of this? Does this have practical implications for training, or for people who want to get into research / self-experimentation? You seem very virtuous to us. What advice would you give to other people who wanted to do self-experiments like this?
Exfatloss: Hm, not sure. I just like experimenting and trying new stuff, I’d probably keep doing it even if I reach my goal weight. Just for fun.
Most experiments have no effect or almost no effect. “It makes no difference” seems the default result.
SMTM: Good insight.
Exfatloss: All diet experiments that somehow rely on you eating less or burning more energy seem to fail very quickly because caloric deficit symptoms set in. I call these diets “inefficient fasts” because you could’ve saved yourself 15 days and gotten too hungry to continue by water fasting, instead of getting too hungry to continue on day 18 of your diet.
Even when you’re really, absolutely, positively sure you identified The Thing, you can be completely wrong. This was my experience after “knowing” through experiment that keto is what made me lose 100lbs. I had literally already written the book 🙂
Lesson in humility. One of the reasons why I’m couching my terms more this time and mostly going off of my experience so far. One of my broader claims this time was the zero-fiber/ketosis thing, and apparently I’ve already been proven wrong. Zing!
I am very critical of Science(tm) as an institution, especially in fat loss and nutrition. It seems that a lot of scientists hide behind mouse models and sophisticated studies so they don’t have to face the fact that nobody actually fricking knows how to lose weight.
Saw a meta-analysis recently that concluded “all diets work well to reduce weight.” Really? Must’ve not heard about this obesity epidemic.
That’s why I love the citizen scientist stuff so much. I think modern ethics boards literally make it illegal to do meaningful diet research.
SMTM: Preach!
Exfatloss: Try getting a 85% calories from heavy cream study approved.
Final Thoughts
SMTM: Finally, can we publish your responses to these questions (and responses to any followup questions) as an interview on our blog? If that sounds good, we’ll produce a version of this email thread, edited for clarity and flow, and go over it with you before publishing.
Exfatloss: Yea, that sounds great! Please edit it to make me sound smart and funny lol. Exfatloss is good as a name. You can mention that I’m a guy just for clarity, as that can make a big difference in fat loss/metabolism I think.
SMTM: How should our readers reach you if they have questions? Comments on your Substack? Email?
And thank you for inspiring me to try this shit again, I had given up until I read the Lithium series.
4 jeans sizes is already so worth it. You wouldn’t believe the quality of life difference 40lbs makes. Literally wouldn’t believe it. If I never lost another pound, this would still be a huge success.
Many chronic illnesses are much more common in women than in men. IBS is about 2-2.5 times more common in women than in men; migraines are about 2-3 times more common; chronic fatigue is about 4 times more common.
This is pretty weird, and more than a little mysterious. And it’s doubly weird that the ratio is pretty similar — each of these examples is about 3 times more common in women than in men.
Normally this gender gap, if it is addressed at all, is written off as a biochemical difference (e.g. here). But another possibility is that gender is just a proxy for body size (e.g. here). If some chronic illnesses are caused by exposure to irritants, heavy metals, or other contaminants, smaller people will generally have more of a response to the same level of exposure, and women on average are smaller than men.
If this is the case, it should be possible to detect if gender is a proxy for body size in some chronic illnesses. If body size is what really matters and gender is just a proxy, larger-than-average women will be underrepresented and smaller-than-average men will be overrepresented. Basically, once you know someone’s height and weight (and maybe % body fat), their gender shouldn’t give you any further information about their likelihood of getting sick.
II.
We can show this with some simulations.
Here’s a simulation of 10,000 men and 10,000 women. The men have an average height of 69 inches with a standard deviation of 3 inches, and the women have an average height of 64 inches with a standard deviation of 3 inches.
Let’s start by seeing what things look like if the greater prevalence of women is the result of something like hormone levels, and body size has nothing to do with it. In this case, the men all have a 1% chance of getting the illness, and the women have a 3% chance. Height doesn’t factor in at all. So when you look at the distribution of heights of men and women in the group of people with the chronic illness, it looks something like this:
As you can see, three times as many women have the illness as men do, but otherwise the distributions are quite generic. These are basically just subsets of the distributions for each gender. They should be normally distributed and should generally look similar to one another, except that there are more women than men and the two groups have different average heights.
Now in comparison, we can consider what the data would look like if gender is just acting as a proxy for height, and there are more women with chronic illness only because they are shorter on average.
Here’s another simulation of 10,000 men and 10,000 women, with the same distributions for height. Without getting into the exact model,[1] this is what it looks like if height is the only thing that determines if you get sick, and shorter people are much more likely to get sick:
Again we see that there are about three times more women than men, even though this time, gender doesn’t have a direct effect. In this simulation, height is the only thing influencing who gets the illness, but the difference in average height is enough to make it so that there are three times as many women as men.
While it’s not clear from just eyeballing the distributions, there are signs in the data that height is driving this difference. For example, about 1% of women are 70 inches or taller in the height-based simulation (compared to about 2.2% in general) and about 9% of men are 63 inches or shorter (compared to about 2.2% in general). This seems like a clear sign that height is the actual thing that determines who gets sick.
III.
Since we don’t know what the real-world dynamics would look like, it’s not clear what you would see in real-world data. It could just be that people with the chronic illness would be shorter on average than people without — American women are about 64 inches tall on average, so it would be interesting if the average height on a chronic illness subreddit was just 61 inches (though you might want to account for age and ethnicity). If the effect was strong or nonlinear enough, there might be a noticeable skew in the data instead. Or you might see the underrepresentation of larger-than-average women and overrepresentation of smaller-than-average men that we describe above.
You could conceivably detect this kind of difference with normal survey methods, as long as you got a large enough sample size. To our mind, evidence that height (or possibly weight, you would want to collect both) explains why women are much more likely to have a chronic illness would be evidence that the chronic illness in question is caused by some kind of contaminant, since other causes shouldn’t be so sensitive to body size. If anyone wants to help collect this data for their community, please contact us.
[1]: The probability of a simulated person getting sick was proportional to 82 inches minus their height in inches, cubed. That is to say, in this model someone who is 56 inches tall was 17,576 times more likely to get sick than someone who is 81 inches tall. These numbers mean nothing, we pulled them out of our ass.
Our psychology is focused on behavior. We focus on behavior because we want to figure out what actions we can take to influence the world around us. But a focus on our actions can also make us superstitious.
The classic example is from a BF Skinner study, where he put a bunch of pigeons in a box and dropped in food at random intervals. Instead of realizing that the food drops were random, the pigeons assumed that they were somehow responsible and tried to figure out what they had done to make the food appear.
Whatever they were doing at the time the food dropped, they tried again. A pigeon who had just turned counterclockwise when the food arrived would turn counterclockwise again and again. When more food eventually did arrive, the counterclockwise-turning was validated. “The experiment might be said to demonstrate a sort of superstition,” wrote Skinner. “The bird behaves as if there were a causal relation between its behavior and the presentation of food, although such a relation is lacking.” [1]
Compare this to a rat confronted with a set of buttons, trying to figure out which of the buttons give food and which give painful electric shocks. Unlike the pigeons, the rat is faced with a deterministic system where her actions lead directly to reward and punishment, so her focus on behavior is justified and leads to a correct understanding of the system. The pigeon is faced with a random system where his actions have nothing to do with the arrival of food, so his focus on behavior is pointless and leads only to superstition and confusion.
so cute though!
II.
We worry this is a common problem in chronic illness. Let’s say that Mary develops chronic fatigue syndrome (CFS). She is proactive and wants to solve the problem, so she comes up with a plan of 26 different treatments, which we’ll call A, B, C, D, and so on. Maybe A is “cut out dairy”, B is “walk 20 minutes every day”, etc. but the specific plans don’t really matter. She starts implementing each plan for two weeks, first plan A, then plan B, etc.
But Mary is working from the wrong assumption. She thinks her chronic fatigue comes from something she’s doing or not doing. In short, she thinks it comes from her behavior. This is a common assumption because our psychology is focused on behavior — we look for things we are doing right or doing wrong. But what really happened is that last month she bought a bag of rice that was grown in a field that was contaminated with cadmium, and developed low-level cadmium poisoning, which is entirely responsible for her chronic fatigue. Cutting out dairy or walking to the corner store won’t do a thing, because the cadmium is the only cause of her illness. None of the interventions she has planned will help.
But the cadmium is slowly being cleared from her system by natural means at the same time as she works her way through the 26 treatments. What happens is this: Mary reaches treatment L (“take omega-3 supplements”) just as the cadmium in her system drops below critical levels, and Mary is immediately “cured”.
Since her symptoms stop almost immediately after starting treatment L, Mary assumes that the omega-3 supplements are what cured her, and continues taking them indefinitely. In reality, the omega-3 supplements do nothing for her — as long as her cadmium levels are low, she doesn’t have CFS, and if she ever gets exposed to high enough levels of cadmium again, her chronic fatigue will come right back.
III.
What Mary should do is she should run a self-experiment with the omega-3 supplements. She should randomly assign some weeks to be on omega-3 supplementation, and some weeks to be off. If she did this, she would quickly find that the omega-3 makes no difference to her chronic fatigue.
It’s understandable why she doesn’t try this — she is worried that if she stops taking the omega-3, her chronic fatigue will come back, and she doesn’t want to risk it. Also, we suspect she wants a world that makes mechanical sense (“I just needed to take more omega-3”) rather than a world where she randomly gets sick and there’s nothing she can do to stop it. It’s hard to blame her for that.
This is how the focus falls on behavior and misses hidden variables. By “behavior”, we mean actions that are directly under people’s control. Eating more or less of something, getting up earlier or later, trying more or different kinds of exercise, and so on. By “hidden variables” we mean essentially any variable you wouldn’t normally think of, especially one not connected to your actions. For example, heavy metals in your drinking water, additives in your food, viruses you contracted from your friends, air pollution from forest fires hundreds of miles away, mold in your ceiling, or things you’re exposed to at work.
Most of these hidden variables can be influenced by your actions, but they’re not the kinds of behaviors that come to mind. You can always quit your job, but for most people, that doesn’t come to mind as a possible treatment for their illness. You can cut out spinach or dairy, because “eat less dairy” is psychologically simple — but “consume less sulfites” isn’t a clear action for most people because “foods with sulfites” isn’t a category to most people. They may not always know which foods contain sulfites, and they may not know what sulfites are.
Does this look like the face of mercy?
IV.
This is what chronic illness looks like for Mary as an individual. At the group level, things look somewhat different.
If a chronic disease is caused by a hidden variable (like cadmium randomly being in some foods but not others), you should see something like this: People get sick for apparently no reason. They all try many different treatments, and most treatments don’t seem to work for anyone. Sometimes a treatment will seem to work for a bit, but then it will unexpectedly stop working. Whenever you feel like you start to get a firm grip on things, all the rules you learn go out the window. However, there are many individual stories of trying some new treatment and suddenly being cured. Unfortunately, the cures in all of these stories are entirely different treatments, and the cures that work for one person never seem to work for anyone else.
And this does sound like what we see in many chronic illnesses, which makes us suspect that some chronic illnesses are being caused by a hidden variable. It could be contamination in food, water, or air, like our hypothetical Mary’s experience with cadmium. But it could also be any other unexpected variable that doesn’t have to do with personal behavior. For example, it could be the result of a virus, or an allergy to something in your household, or a curse put on you by the local witch. When taken as a group, chronic illness communities look exactly how we would expect them to look if the illnesses were caused by some hidden variable, and that makes us suspect that they are caused by some hidden variable.
Naturally this makes us wonder if there is any way to figure out what these hidden variables might be, assuming you believe they exist. The fact that they are hidden does make it inherently tricky, but we have a couple of ideas, here they are.
TRY BIG ELIMINATIONS
Your chronic illness may be triggered by something in your environment (your home, work, local food, local water, etc.). To test this, you can change as much of your environment as possible all at the same time, for example by taking an extended trip to Nepal.
If you start feeling better or your symptoms disappear, this strongly suggests that something in your home environment is causing your illness. If you don’t feel any better, it suggests that your symptoms 1) aren’t caused by your environment, 2) are caused by elements of your environment that you brought with you (e.g. your clothes, your shampoo), or 3) are caused by elements of your environment that are common to both your home and Nepal (car exhaust?).
Your chronic illness might also be triggered by something you eat. To test this, you can change as much of your diet as possible all at the same time, for example by trying the potato diet, where you eat essentially nothing but potatoes. The potato diet is good because potatoes are simple, contain no additives, and are more or less nutritionally complete. Many people can survive happily on nothing but potatoes, salt, water, and hot sauce for up to four weeks (we have good data on this!).
If your symptoms disappear or get better, this strongly suggests that either you had some deficiency that the potato diet fixed, or something in your normal diet is causing your illness. If your illness is just as bad as ever, it suggests that either your symptoms aren’t caused by your diet, or are caused by elements of your diet that are also in the potato diet.
Neither of these approaches will tell you what is causing your illness, but both have the potential to narrow things down enormously. If you go to Finland for a month and your migraines stop three days in and don’t come back until you get home, that’s pretty clear evidence that something at home is causing your migraines. You don’t know if it’s your laundry detergent, your well water, or something at your job, but you can take steps to narrow it down further, and you can stop worrying about your diet so much.
Similarly, if you try the potato diet for a month and your executive function issues disappear, you can stop worrying about fumes from your boiler and can try to figure out what part of your diet is giving you brainfog.
Even a null result is informative. If you go on the potato diet for a month and your migraines carry on as normal, that’s a pretty clear sign that it’s not something in your diet, and you should look elsewhere.
Some people find this approach surprising, because scientific investigation usually involves isolating a small number of variables and putting them under tight control. This works fine when you have a small number of variables to start with, or you know which variables you’re interested in. But in the search for hidden variables, there are a nearly infinite number of things that could be the cause of your illness. We need a technique that lets us rule out lots of theories at once, so doing these big splits can be extremely productive.
There’s a classic genre of logic puzzles often called balance puzzles. In these puzzles you have several coins, one of which is lighter than all the others, and you have to use a balance scale to find the light coin in the smallest number of weighings. The way you solve these problems is by splitting the coins into groups and comparing the groups directly. If you split the coins into two groups and the group on the right weighs less than the group on the left, the light coin must be in that group.
spoilers
Consider a version of this puzzle where there is an illuminated lightbulb and a row of 1,000 switches. You want to find the switch that controls the lightbulb, but you don’t know which it is. You could go down the row of switches and try them one by one, but this would probably take you several hundred steps. On the other hand, if you have some kind of opportunity to flip a bunch of switches at once, that can narrow things down really quickly.
Let’s say that half the switches are red and half are blue, and you can flip all the switches of a single color at once. If you flip all the red switches and the light goes off, then the master switch must be red. If you flip all the red switches and the light stays on, then the master switch must be blue. Either way, you now have only 500 switches to try.
This is the same situation we’re in with chronic illness, except that there are something like 1,000,000 switches on the wall, and in some cases the lightbulb might be controlled by complicated interactions between multiple switches. It still makes sense to toggle big groups of switches all at once when you can, because that can narrow things down drastically.
One limitation of this approach is that it’s only really good at finding triggers. If you’re suffering from an iron deficiency, big eliminations probably won’t help find that.
The other limitation of this approach is that it’s not always clear how long you have to eliminate things for. Do you need to eliminate the mystery trigger for a week? A month? Longer? Ideally we could send you to Nepal for a year, or put you on the potato diet for a year, but in reality this won’t be practical for most people.
If Mary is getting poisoned by cadmium, and it takes two months to clear all the cadmium from her system, then going on a restrictive diet for only one month won’t help. But the problem is, she can’t know this in advance. How is she supposed to know about the clearance rate when she doesn’t even know what’s poisoning her?
So we’re stuck with an asymmetry. If one of these eliminations helps you, that narrows things down quite a bit. But if they don’t help you, then it’s more ambiguous. Maybe the half-life of whatever is making you sick is just too long. Still, it seems like it would be worth trying.
TRY SOME LIKELY VARIABLES AT RANDOM
Another possibility is to just try various things and see what works. This is grasping in the dark, but we can still do a lot to cover our bases.
For example, there are a finite number of vitamins. “Vitamin deficiency” is a plausible type of hidden variable, so you could just cycle through all the vitamins and see if any of them happen to be an immediate cure. It seems unlikely that you will get this kind of miracle result, but vitamins are pretty safe so the risk is very low, and you could at least check “vitamin deficiency” off your list.
Similarly, there are a finite number of elements. Some of them, like iron and potassium, are necessary for human health. You could try supplementing these and see if that treats your illness. Other elements, like lead and mercury, are known to be bad for your health. You could try getting blood and/or urine tests, or testing your local water supply, and see if you have higher exposure to any of these known toxins.
Again these are all shots in the dark, but they’re all plausible variables that could be affecting your health. If it turns out your blood mercury levels are way higher than normal, that would be good to know.
You could also try to hit your illness with some generic treatments, basically anything where the name starts with the prefix “anti-”. If you can convince your doctor, you could maybe get them to put you on a broad-spectrum antibiotic (in case your chronic illness is bacterial), antiviral (in case your chronic illness is… etc.), antifungal, anti-inflammatory, or antihistamine. This is a little more risky, but there’s some chance your chronic illness might be fungal and this is one of the only ways you would ever find out.
This broad-spectrum approach will generally be better for finding deficiencies, but in some cases it might also help identify triggers.
GET RID OF YOUR BLOOD
Haha, but no, seriously. Donating blood is easy, safe, and it’s a nice thing to do for your community. You might save a life. And if there’s something nasty building up in your blood, you might be able to get rid of some of it. There’s already some evidence that donating blood can reduce your serum PFAS levels. Maybe it can clear some other things from your system.
Again, this is a pretty blind approach. It probably won’t work for most people. It may not work for anyone at all. But if you donate blood and your symptoms immediately get better, that would be pretty interesting, right?
V.
In the beginning, we’ll be taking shots in the dark. People will try dozens of things with little or no success. This will be quite frustrating.
But the hope is that eventually, we will start to get our bearings. If a couple people with chronic fatigue find that they have high levels of cadmium in their blood, then other people with chronic fatigue will want to check their cadmium levels before trying other interventions. Conversely, if a couple dozen people with chronic fatigue check for cadmium and find nothing, checking for cadmium should be moved lower down on the list for chronic fatigue.
Depending on the success of this approach, you can even imagine this being somewhat formalized. Someone could make a centralized list of things to try or to have tested, and people could report what they had tried and whether it worked out. Tests that seem to be helpful could be moved up in the rankings so people could know to try them first; tests that don’t seem to help people could be moved down and left for the last ditch attempt.
Will this work at all? Who knows, but it seems like it’s worth trying. And at the very least, we may be able to rule out some hypotheses. After all, if we can establish that it’s none of the things on this list… then what the hell is it?
Endnotes
[1]:
“A pigeon is brought to a stable state of hunger by reducing it to 75 percent of its weight when well fed. It is put into an experimental cage for a few minutes each day. A food hopper attached to the cage may be swung into place so that the pigeon can eat from it. A solenoid and a timing relay hold the hopper in place for five sec. at each reinforcement.
If a clock is now arranged to present the food hopper at regular intervals with no reference whatsoever to the bird’s behavior, operant conditioning usually takes place. In six out of eight cases the resulting responses were so clearly defined that two observers could agree perfectly in counting instances. One bird was conditioned to turn counter-clockwise about the cage, making two or three turns between reinforcements. Another repeatedly thrust its head into one of the upper corners of the cage. A third developed a ‘tossing’ response, as if placing its head beneath an invisible bar and lifting it repeatedly. Two birds developed a pendulum motion of the head and body, in which the head was extended forward and swung from right to left with a sharp movement followed by a somewhat slower return. The body generally followed the movement and a few steps might be taken when it was extensive. Another bird was conditioned to make incomplete pecking or brushing movements directed toward but not touching the floor. None of these responses appeared in any noticeable strength during adaptation to the cage or until the food hopper was periodically presented. In the remaining two cases, conditioned responses were not clearly marked.
The conditioning process is usually obvious. The bird happens to be executing some response as the hopper appears; as a result it tends to repeat this response. If the interval before the next presentation is not so great that extinction takes place, a second ‘contingency’ is probable. This strengthens the response still further and subsequent reinforcement becomes more probable. It is true that some responses go unreinforced and some reinforcements appear when the response has not just been made, but the net result is the development of a considerable state of strength.”