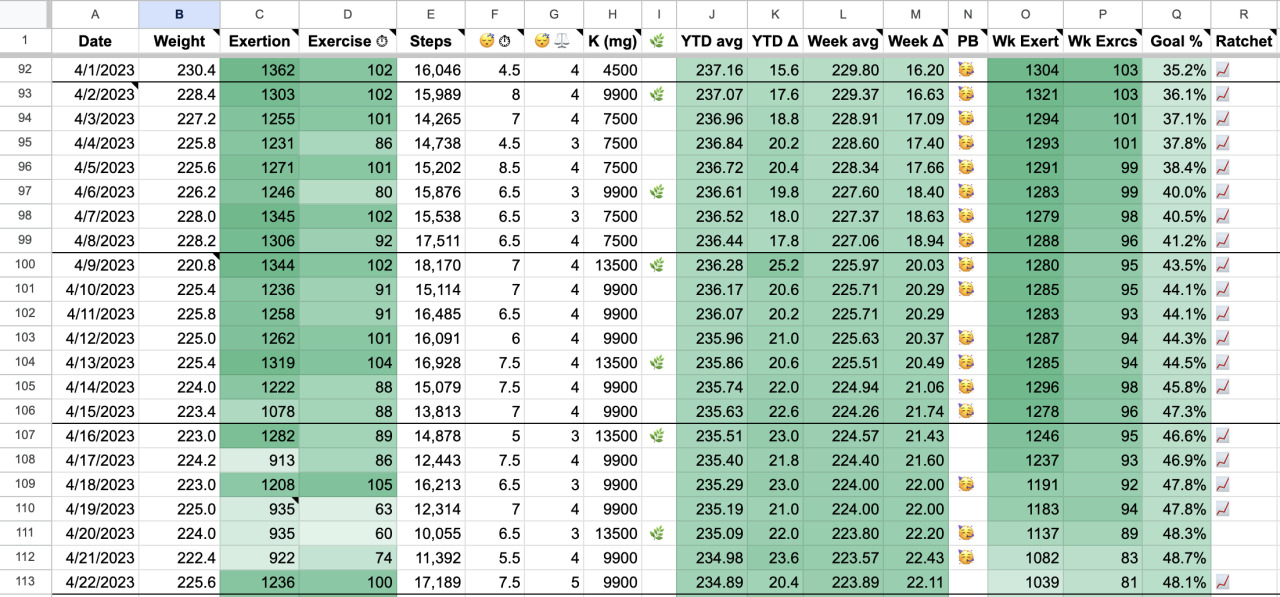
Krinn also added an exercise habit that she described as a “naïve just-hit-the-treadmill exercise regimen”. Even with this in mind, her results still seem remarkable, because most people do not lose 50 lbs from starting a moderate treadmill habit:
We published a short review of that original post on this here blog of ours. That was in July 2023. Now, Krinn is back, and more powerful than ever, with an untitled post we’ll call A Year And Change After The Long Post About The Potassium Experiment (AYACATLPATPE).
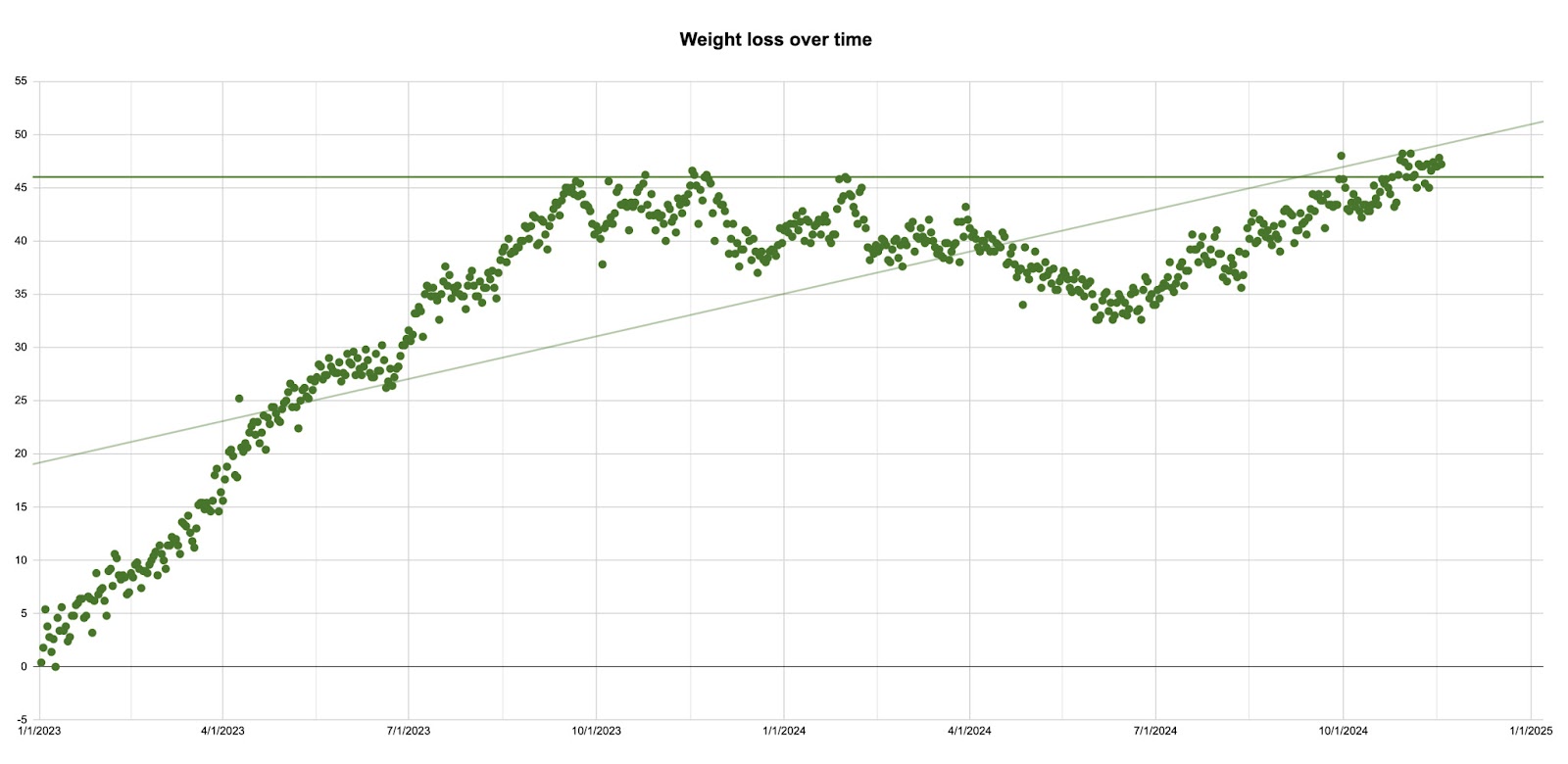
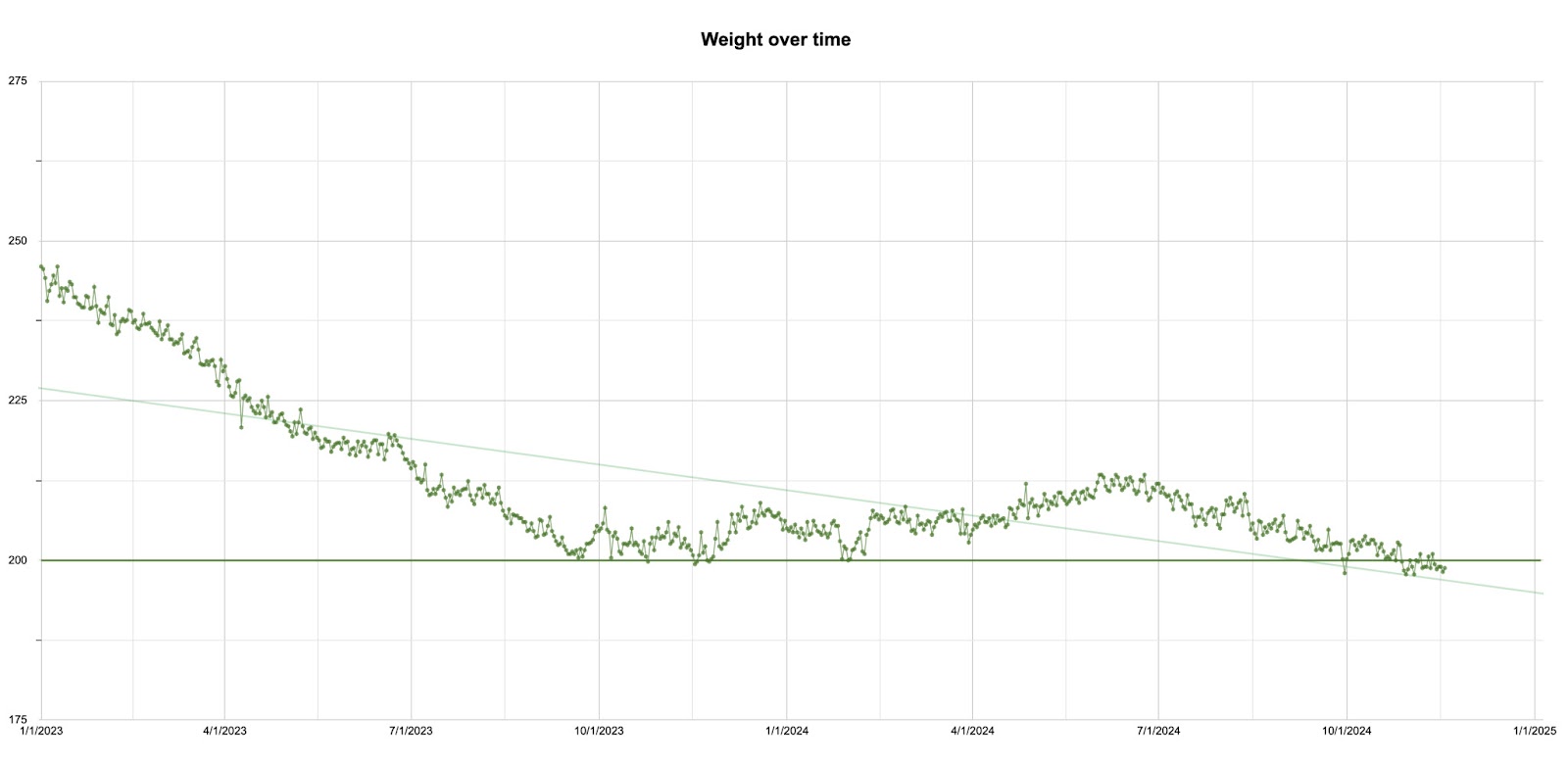
The long and short of it is that Krinn kept taking high doses of potassium and kept losing weight, eventually reaching her goal of 200 lbs. There was a long plateau in the middle after she first brushed up against her goal, but she maintained the original weight loss and eventually lost the remaining weight:
In personal communication (see very bottom of this post), Krinn noted that:
One of the few things the graphs say really, really, really loudly is “Krinn lost 30+ pounds _and stayed that way for at least a year._” … one of the overwhelmingly common failure modes of existing interventions: people lose some weight and then gain some weight and end up fairly close to where they started. Whatever else happened in my experiment, it sure wasn’t that: I lost a significant amount of weight and then _stabilized._ That seems important.
This time we don’t have much to add, but as before we wanted to reproduce her post for posterity. And we do have a few thoughts, mainly:
This seems like more evidence that high doses of potassium cause weight loss. It suggests that potassium is probably one of the active ingredients, maybe the only active ingredient, in the weight loss caused by the potato diet. Krinn was taking about as much potassium as you would get if you were eating 2000 calories of potatoes per day, and experienced similar weight loss.
It’s good to be skeptical of single case studies, however rigorous and careful they may be, but here are a few things to keep in mind:
Remember that participants in the Low-Dose Potassium Community Trial lost a small but statistically significant amount of weight (p = .014) on a dose much lower than what Krinn was taking — only about 2,000 mg of potassium a day on average, compared to Krinn’s ~10,000 mg per day. This can’t confirm the effects of the higher dose, but it is consistent with Krinn’s results, and the final sample size was 104 people.
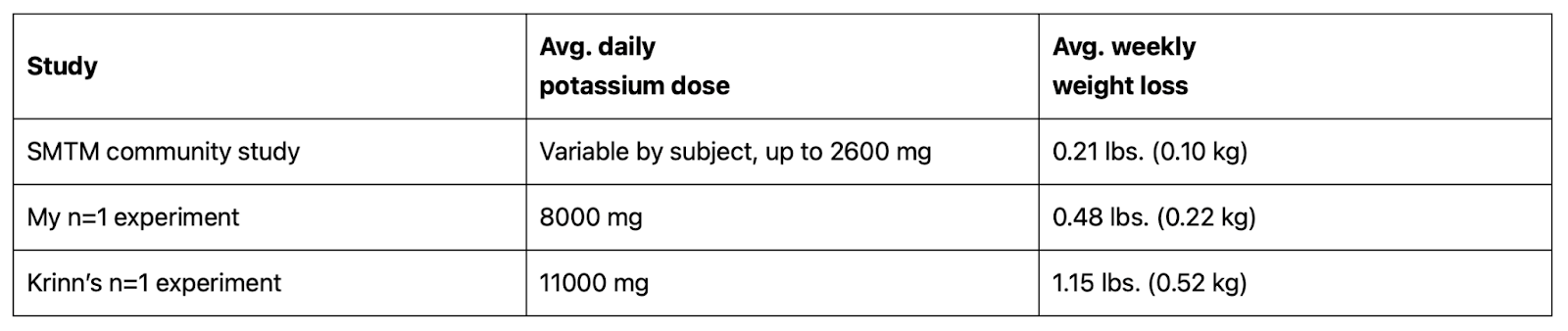
There’s also at least one successful replication. Inspired by Krinn’s first report, Alex Chernavsky did a shorter potassium self-experiment and lost about 4 pounds over a two-month period, otherwise keeping his diet and exercise constant. He also provided this handy table:
Finally, we know of two other people who are losing weight on high-potassium brines, at least one of them without any additional exercise. They’re both interested in publishing their results, probably in early 2025. So watch this space. :)
As before, we want to conclude by saying that Krinn is a hero and a pioneer. She is worth a hundred of the book-swallowers who can only comment and couldn’t collect a data point to save their life. If you want to do anything remotely like what Krinn did, please feel free to reach out, we’d be happy to help.
Here’s a reproduction of Krinn’s full report as it appears in her tumblr post:
A Year And Change After The Long Post About The Potassium Experiment
A year and change after the long post about the potassium experiment, I reached my weight-loss goal. This is a quick, minimally-structured thought-dump about it. As before, this is part of a wider conversation that starts with A Chemical Hunger.
Methodology: I mostly kept doing what I’d been doing. Turned up the exercise dial a bit, turned down the potassium dial a bit. Both still, AIUI, quite high compared to American baseline. Some bad news — in addition to whatever confounding factors were present last time, there’s a few extra ones now from my life in general going very poorly. As before, here’s the data, Creative Commons Zero, good luck with whatever you try on it. After making it to one year of being fairly diligent, I decided to let things vary and see what happened — on the one hand, I’d gotten far enough towards my personal goal that I wasn’t too fussed about the last 10%, and on the other hand, if this works in general and even work when you’re kinda half-assing it, that too is great news.
Interpretations: There’s multiple ways this could go. Here are a few that were easy to think of.
Potassium or potassium-plus-exercise caused me to lose weight
Exercise caused me to lose weight and potassium was irrelevant
Something else caused me to lose weight
I would prefer to believe that potassium-plus-exercise caused me to lose weight. The data I have and my experience of gathering/being that data, to some extent support that conclusion. Flipping that around, if I ask “does that data rule out this conclusion?” no it absolutely does not. But it’s important to note that the exercise-only conclusion is only slightly less-well-supported and the none-of-the-above explanation is much-less-well-supported but certainly not ruled out. I have a preferred explanation, but all three of these explanations are live.
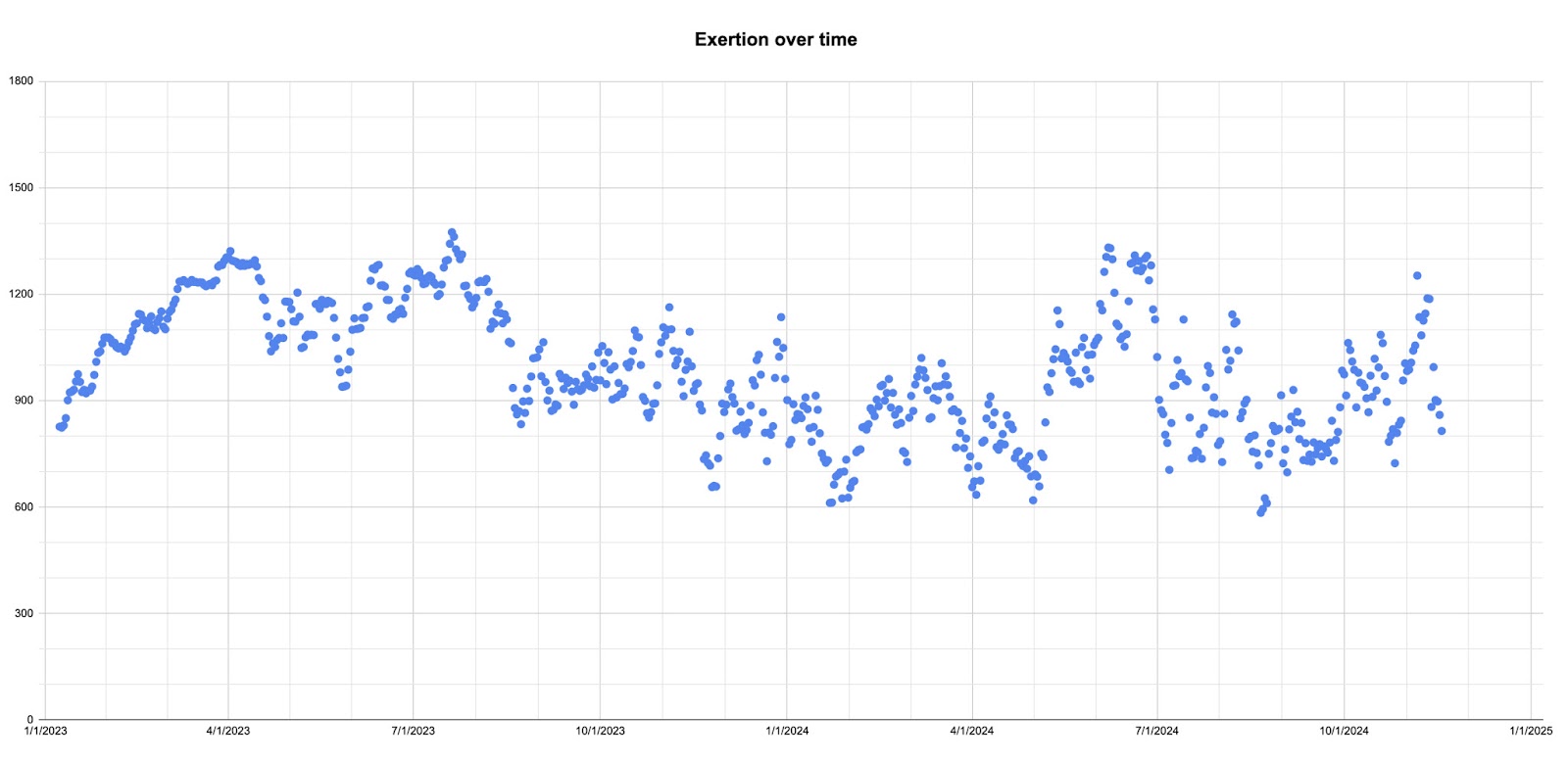
My subjective experience of the thing was that there was an easy part and a hard part. In the easy part I lost weight at a pretty rapid and consistent pace. In the hard part, my weight changed less and went back and forth more than it went down. If you buy into SMTM’s “something is screwing up people’s lipostats” theory, this is very consistent with that theory: potassium reduced or removed the something, my weight briskly dropped back to a healthy range (the first 9 months of the graphs) and then stabilized. However, the competing theory of “Krinn was super out of shape and then she started exercising” is also supported by the graphs (not shown on the graphs: my fairly poor 2022 exercise habits — my long-term exercise habits have had some good stretches, but the plague years did not do good things for me there!). I’m not sure whether it matters that I shifted from mostly treadmill time to having a couple of walks around the neighborhood that I can do pretty much on autopilot (shout-out to Mike Duncan’s Revolutions, this show is the first time podcast as a medium has clicked for me and it’s a great show). I do think, though, that exercise is a bit more complicated than I was really grasping. That, in turn, makes me glad that I’m tracking three exercise metrics rather than just one — if I was going to track only one, it’d be exertion, but exertion, exercise minutes, and step count, together make it possible to at least take a guess at what qualities a day’s exercise had.
Regarding my own questions from the first post:
• How safe is this? When I made the first post I was antsy about “adding this much potassium to your diet is probably safe for people in generally good health” but now I’m pretty sure it’s true. Some health problems can take a long time to present themselves, but adding this much of something to your diet for two years and having it be fine, is pretty persuasive evidence that the thing is probably fine. It could still easily turn out to have negative health impacts that are important, but a huge swath of the things you’d be worried about, are vanishingly unlikely once you’ve hit the point of “I’ve been taking this for two years and I’m fine.”
• Does this replicate? Well, it’s self-consistent for me, and I don’t want to gain 50 pounds and try again. I did not like the shape of my body at +50 pounds from where I am now! So this is a question for others.
• How much do other nutrients matter? I don’t know. Mostly not equipped to rigorously check.
• Does HRT matter? I’ll let you know if I can get back on HRT. I would definitely like to investigate this.
• Does dieting matter? Probably: my diet changed involuntarily over the course of two years and that certainly matters to some extent, but one of my ground rules is that I’m focusing on controlling exercise and potassium, the things I can control. Diet is far more complex and also in my life particularly, more susceptible to unplanned, involuntary change, so I’m writing it off as a factor.
• Does this help with cannabis-induced hunger? I think I was off-base/over-optimistic with this one and it either doesn’t matter or matters a small amount.
• Is there a point where I get really hungry/tired or start accidentally starving? I did not reach such a point. I felt basically fine the whole time.
I was cooking with this though:
If you tell someone you want to lose weight and would like their advice, it is overwhelmingly likely that the advice will involve exercising more. Everyone has heard this advice. And yet, as Michael Hobbes observes in a searing piece for Highline, “many ‘failed’ obesity interventions are successful eat-healthier-and-exercise-more interventions” that simply didn’t result in weight loss. Even if we as a society choose to believe “more exercise always leads to weight loss, most people just fuck up at it,” that immediately confronts us with the important question, why do they fuck up at it? and its equally urgent sibling, what can we learn from those who succeed at it to give a hand up to those who have not yet succeeded?
Conclusion: I’m gonna keep writing things down in my spreadsheet for the same reasons as last time. I’m not sure what exactly I’m going to do as far as twiddling the factors, because now my main goal is somewhere between “don’t gain weight again” and “see what happens,” but I do know that writing down what happens is Good Actually, so I’m going to keep doing that.
Slightly after publication, Krinn sent us these comments, which she agreed we could publish:
Personal Communication
Dangit now I’m having the first draft effect: writing the first draft and sleeping on it tells me things I should have written. In this case, I think there’s a plausible reading that my experience supports the “potassium does something good at a high enough effect size to care about” line of argument because while the peaks of how much effort I put in were fairly high — the periods of combined high exercise and high potassium intake — the most noticeable effect was when I was ramping up on both of those in the first 9 months, and when I was in just-bumbling-through-like-an-average-human mode, the effect didn’t reverse itself. There were plateau periods and there were slow-reversion periods, but there was definitely no “you slacked off and now there’s rapid weight gain mirroring the rapid weight loss” effect. I think that’s positive? I think it’s plausible to read it as “once I got the majority of the weight loss effect, locking in that benefit was easy.”
In any case one of the questions I was interested in was “if this works, does it work well enough that an average person can successfully implement it?” and I am now convinced that that’s a clear “Yes”.
I wouldn’t say there’s any part of this experiment that I’m actively unhappy about, but I do find it a little frustrating that this is basically just another piece of evidence on the pile of “here’s something that is consistent with the lithium/potassium hypothesis, but that is also consistent with some other stuff, and my main observation is that Something Happened” — intellectually I feel sure that much solid science is built by assembling big enough piles of such evidence and then distilling it into “now we know Why Something Happened,” but putting one single bit of evidence on the pile is still something where I need to make my own satisfaction about it rather than having a well-established cultural narrative rushing to bring me “yes! you did the thing! Woohoo!”
Also thinking more about the potassium experiment I’m having one of those “hold on a minute, this should have been obvious to me” moments — one of the few things the graphs say really, really, really loudly is “Krinn lost 30+ pounds and stayed that way for at least a year.” That’s one of the crucial parts of the whole obesity thing, that second half, right? That’s one of the overwhelmingly common failure modes of existing intervention: people lose some weight and then gain some weight and end up fairly close to where they started. Whatever else happened in my experiment, it sure wasn’t that: I lost a significant amount of weight and then stabilized. That seems important.
Yessssss I get the smug clever-kitty feeling, this is exactly why I have that “ratchet” column in the spreadsheet: the last ratchet-tick day from more than a year ago (i.e. it’s locked in) was July 10th 2023, on which day my week-average weight was 212.4lbs, down 33.6lbs from the start of the year.
So that early period of dramatic weight loss is noteworthy because we can be confident that whatever the cause was — potassium, exercise, or something else — it caused durable weight loss, which is exactly the thing we are looking for.
This is a conclusion we couldn’t have reached in July 2023, with the major writeup I did, because at that point “something else happens and Krinn gains the weight back” was very possible, was one of the likely answers to “what comes next?”
JV is a reader and intrepid high-dimensional pioneer who wrote us with some thoughts and comments on the exploration of brinespace. His email is reproduced below, lightly edited for clarity and to help preserve anonymity, but otherwise the same as we received it.
Hello Slimes
I’m a long time reader of your blog and greatly enjoyed your recent post wrt. explorations of brine space. I’ve engaged in somewhat similar experiments due to some health problems (IBS-D is a likely diagnosis but I’m still hoping for something a bit more actionable). Particularly, I had some temporary success about a year ago experimenting with potassium chloride which greatly improved my wellbeing for about two weeks but then, unfortunately, it stopped working. My experiment was similar to Krinn’s in terms of dosage but with the crucial difference that I did not add sugar to the solution. I now understand, thanks to several of your recent blogs and references therein, why this may have caused my experiment to fail.
I’ve decided to give potassium chloride another go, using Krinn’s experiment as a point of departure. In considering the optimal experimental strategy for searching brine space, I conducted a brief mathematical exercise that I think may interest you as well. My brief experiment can be replicated in the attached python script.
I should probably mention somewhere, that I’m a complete ignoramus wrt. chemistry, so this is a purely mathematical exercise with all the attendant risks of making stupid chemistry 101-level conceptual mistakes.
Anyway, I jumped right in and tried to replicate Krinn’s solution. I don’t have Gatorade easily available, so I used normal lemonade and added roughly two teaspoons of potassium chloride to 1 liter of water along with the normal amount of lemonade (1:4 mixing ratio) and a teaspoon of salt. In short order, I discovered two things: ingesting the solution 1) made me feel better and greatly reduced my appetite (yay!) and 2) made several subsequent visits to the bathroom urgently necessary (boo!). Reading a bit more about the formulation of ORS explained the latter phenomenon: I had inadvertently made a hypertonic solution, meaning that solution drew water into the intestines due to the osmotic gradient. Apparently, this amount of water was such that it could not be reabsorbed. Thus, I arrived at the conclusion that I should make future solutions isotonic (i.e. eliminate the osmotic gradient) or, like the more recent formulation of ORS, slightly hypotonic to facilitate absorption of the mineral salts.
You may have encountered the formulation of the reduced osmolarity ORS with an slightly hypotonic osmolarity of 245 mOsm/l relative to the previous formation with isotonic osmolarity of 311 mOsm/l (https://www.rehydrate.org/ors/low-osmolarity-ors.htm). It makes sense, to me personally, that the optimal tonicity of any ingested solution should be somewhere in this interval. After all, hypertonic solutions have the major disadvantage that the ingested mineral salts are rapidly excreted, rendering them useless. And so, I assume that any experimental brines should be, at the very least, isotonic but, probably, somewhat hypotonic to facilitate easy absorption. If this assumption is correct, it would have the major advantage, that it significantly reduces the amount of brine space that we need to investigate as the subset of ideally hypotonic brine space (say 245 mOsm/l) is much smaller.
First, I created a script to calculate the osmolarity of Krinn’s solution. In the attached script, the amounts correspond to the ingredients in blue gatorade which result in a calculated osmolarity of 245.6 mOsm/l. I assume it is no coincidence that this closely mirrors the osmolarity of the recent formulation of ORS and, in fact, googling the osmolarity of gatorade, I encountered several criticism of the osmolarity of Gatorade from 10-15 years ago, so I assume the formulation was changed in response.
Of course, this means that adding two heaping teaspoons (slightly less as Krinn was adding them to 20 oz bottles) creates a severely hypertonic solution, which explains my experience with my attempt at Krinn’s solution. This is in no way a criticism of Krinn’s post and, in particular, I note that she writes that she “sips” the solution during the day, which probably explains why she didn’t have any issues. For myself, however, I think it’s better idea to make a hypotonic solution so that I can drink as much as I want.
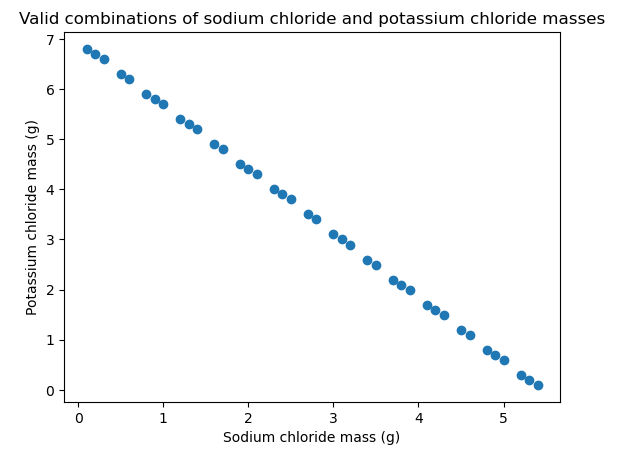
Second, I created a script to identify the optimally hypotonic subset of brine space in a solution of sugar, salt and potassium chloride. That is, I assume a certain target osmolarity (245 mOsm/l) and amount of sugar (20 g/l) and find the combinations of salt and potassium chloride that results in the optimally hypotonic solution. The result is illustrated below, showing me that I should use quite a bit less of both minerals, close to perhaps 1 teaspoon of potassium chloride and maybe 1/5 teaspoon of salt per liter.
Third, I created a script to do the same for three minerals, using calcium chloride as an example but you could use any mineral salt, really.
Based on these experiments, I conclude that the assumption of the optimally hypotonic solution leads to a subset of brine space that is a linear plane, which should drastically limit the combinations to investigate.
Anyway, I hope you find this interesting and/or useful. At any rate, this is the approach I will take to exploring brine space. If I make any further progress, I’ll let you know.
If you wish, you may freely use or reference this material and the attached script.
Cholera gives you severe diarrhea, which leads to agonizing, life-threatening dehydration.
Doctors long realized that cholera patients needed electrolytes, but electrolyte solutions didn’t seem to help.In fact, giving patients electrolytes in IV or in an oral solution often made them worse.
After decades of trial and error, they discovered a mixture of water, electrolytes, and sugar that would treat the dehydration from cholera instead of making it worse. This brine came to be known as oral rehydration solution (ORS), and is now the standard treatment for extreme dehydration.
Why did [early attempts] at oral rehydration fail? It seems that the scientist[s] didn’t yet know some of the fundamental biology of how glucose and sodium was absorbed in the body. Work in the late 1950s and early 1960s had established that sugar and sodium ions are absorbed together in the gut through a sodium-glucose cotransport protein. In turn, this sodium and glucose pulls water from the gut into the body.
Another surprise is that you need to get the solution just right. You can’t just pick a random point in brinespace. As researcher Robert Allan Phillips discovered, if you choose the wrong ratio of ingredients, you kill your patients instead:
The trial was a disaster. When Phillips returned to Manila a week later he was told that five of his 30 trial participants had died. It’s not clear exactly what went wrong with Phillips’ experiment, but we do know that the oral solution he put together had far too much glucose and salt. This made the solution extremely hypertonic — it drew water out of the patients’ cells and exacerbated their dehydration.
Functional solutions for cholera exist only in a relatively small range. Go too far outside that range, and the solution hurts your patients instead of helping them.
We don’t know how narrow that range really is. But we do know you have to get the mix right, or it doesn’t work.
II.
Any combination of electrolytes in solution can be expressed as a point in high-dimensional brinespace.
We begin with a liter of water, the origin along all dimensions. A simple brinespace might define a brine by the concentrations of sodium and potassium per liter, written as [mg Na, mg K].
The point [100, 100] would indicate a brine that contains 100 mg each of sodium and potassium per liter of water. Official concoctions of ORS are more complex, but the simplest make-it-at home version of ORS is located at the point [1150, 0].
But that’s not quite right, is it? ORS contains other ingredients than just sodium and water. Most notable is sugar. If we define a new brinespace of [mg Na, mg K, g sugars], then ORS is located at [1150, 0, 25].
Gatorade is another simple brine. With 270 mg sodium, 80 mg potassium, and 34 g of sugar in a 20 oz bottle, it can easily be defined as the brine at [460, 135, 60] (with some rounding).
One “stick” of the electrolyte mix LMNT contains 1000 mg sodium, 200 mg potassium, and 60 mg magnesium. We’ll have to add magnesium to our brinespace, which we’ll now define as [mg Na, mg K, mg Mg, g sugars]. They recommend you mix this with “anywhere from 16 to 32oz of water”. Given that 32 oz is approximately a liter, this means that LMNT produces brines approximately along the line from [2000, 400, 120, 0] to [1000, 200, 60, 0].
Other electrolyte drinks can be characterized the same way. LiquidIV is located at [1060, 780, 0, 25]. Pedialyte is almost the same (at least in terms of these dimensions), resting near [1030, 780, 0, 25]. Propel (a Gatorade product), has no sugar and can be found at the coordinates [460, 120, 0, 0].
The location of “snake juice” is left as an exercise for the reader.
Even Red Bull is something of a brine. If we define a new brinespace that includes caffeine [mg Na, mg K, mg Mg, g sugars, mg caffeine], then Red Bull is located at approximately [420, 0, 0, 110, 320].
Red Bull isn’t even that unique for having caffeine. Thirst Quencher 2 (TQ2), the forbidden sequel to Gatorade, itself contains caffeine. While Quaker Oats sued to take ownership of TQ2, and then buried it forever such that it has never seen commercial release, we have what appears to be the patent, which defines TQ2 pretty well. Ignoring the phosphate, glycerol, and pyruvate for the moment, we can use the same brinespace as Red Bull. In terms of this brinespace, TQ2 appears to be at about [600, 80, 0, 40, 150], compared to standard Gatorade at [460, 135, 0, 60, 0].
TQ2 makes it pretty clear that the only sugar it contains is glucose, while in standard Gatorade the sugar is some combination of sucrose (50% glucose and 50% fructose) and dextrose. In case that makes a difference, and assuming for the moment that standard Gatorade contains only sucrose, we might want to define a new brinespace [mg Na, mg K, mg Mg, g glucose, g fructose, mg caffeine], in which case TQ2 is located around [600, 80, 0, 40, 0, 150], with standard Gatorade at [460, 135, 0, 30, 30, 0].
(This makes us wonder if glucose is functionally different than other sugars. ORS recipes specify glucose, which suggests that other sugars might not work. TQ2 claims to be an improvement on Gatorade and also specifies glucose. Does fructose not fill the same functions? Is there no sodium-fructose cotransport protein?)
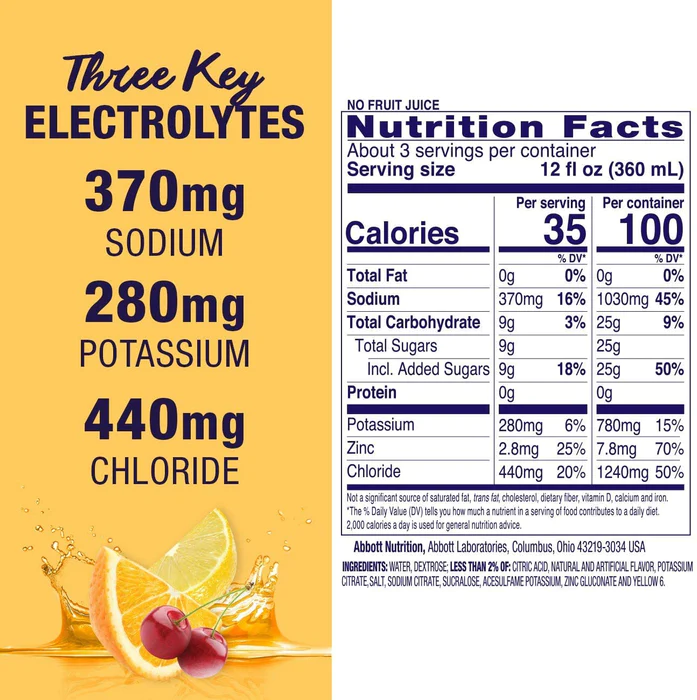
The astute reader will have noticed that all the ions we’ve been talking about up to this point are cations. What’s up with that? Is there some kind of big prejudice against anions? Of all the mixes we’ve looked at so far, Pedialyte is the only one that lists chloride on its nutrition facts label, though most electrolyte solutions presumably have some chloride, since most use NaCl or KCl. Pedialyte in fact gives a percent daily value of chloride (440 mg is apparently 20% DV). We had no idea chloride even had a recommended daily value. But it is in fact an essential electrolyte — without it, you die.
Or how about iodine? That’s an essential electrolyte, it’s a anion (as iodide), but it’s never added to electrolyte drinks, never mentioned on nutrition labels. Maybe people don’t want to hear about chloride ions in their Gatorade, because it makes Gatorade sound like it’s chlorinated (which in some sense, it is), but why not iodide? Any electrolyte mix that includes iodized salt will contain both iodide and chloride, and both of them are biologically active.
Anyways, good on the Pedialyte team for being the exception
A brine might contain any number of other ingredients, and these don’t necessarily need to be electrolytes or sugars.
For example, you could define a brinespace that includes some acids. Ascorbic acid (AKA vitamin C) would be one natural choice — in this case, your brine would cure scurvy. You could also include citric acid. This is certainly found in lemonade, though it’s not clear whether it’s an active ingredient in that context.
Or how about acetic acid, better known as vinegar? The health benefits are controversial, but there are many cultural drinks that are basically just sugar + acetic acid. The ancient Greeks had oxymel, the Romans had posca. Persians have sekanjabin, England gave us “shrubs“, and New England has switchel. Lots of cultures seemed to settle on this combination independently, and kept with it for hundreds of years. Maybe there’s something to it.
Even Milk is a brine. It contains sodium and potassium, calcium, sugars, even iron. It’s an unusually complex brine, sure, but a brine nonetheless.
malk
III.
Some brines have health and wellness benefits.
ORS is the clearest example. Brines from the correct region of brinespace provide a fast and effective treatment for the intense dehydration of cholera. Go too far outside of that region of brinespace, and the brines stop working, then start making the patients worse — some brines will even kill them. It doesn’t work if the ratios are off! Finding the correct location in brinespace matters a lot.
While ORS is exceptional, we don’t think it’s unique. For starters, we have anecdotes like this one:
The extreme version of “grogginess on waking” is hangovers. If you take Pedialyte for hangovers, you are already brining. The company also believes in this application — they recently released a formulation for just that situation.
Sports drinks are another obvious example. Gatorade makes $7 billion in sales per year. Either Gatorade provides some kind of benefit, or their marketing team deserves a raise.
And there are the direct testimonials. Robb Wolf, the co-founder of LMNT, says:
Salt-deprived rats are sad. They loaf around their cages, ignoring the sugar water that usually brings them joy. It’s classic depressed behavior.
I unwittingly ran a similar experiment on myself for the better part of 20 years. I was sweating buckets—unlike pigs, who don’t actually sweat by the way—on the jiu-jitsu mat, but wasn’t consuming enough sodium to replace my losses. I felt low-energy, foggy, and, as I think back, losing passion for my sport. I wasn’t giving my body what it needed, and my mood paid the price. Getting more salt was the remedy.
Compared to other factors, the link between sodium status and mood isn’t well-publicized. I want to change that. I’m not saying salt is a cure for depression, but I do believe it’s worth considering as part of a holistic approach to mood maintenance. Mental health is the fruit of many inputs. And oftentimes many things are out of our control, but getting enough sodium isn’t one of them.
If Robb is right, then some cases of “depression” might just be a chronic lack of electrolytes. This would be simple to test.
Like ORS, Robb also claims that the wrong mix of electrolytes doesn’t work. In our terms, you need to find the correct point, or at least the correct region, in brinespace.
POPULAR PRODUCTS DIDN’T CUT IT. … When I dialed in the formulation I immediately felt my fitness, sleep, and brain functioning on new levels.
Sodium and glucose aren’t the only ingredients where you need to get the mix right. One of our friends, a physician, pointed out that for patients with low potassium (hypoK), if you don’t have enough magnesium (hypoMg), you’ll be hypoK forever unless you fix the hypoMg first, because of “some renal excretion thing I think” (his words). See also this paper, which says: “magnesium replacement is often necessary before hypokalemia and potassium depletion can be satisfactorily corrected with potassium supplements.”
Of course, most regions of any brinespace are going to be unremarkable, or slightly dehydrating. But there are reasons to suspect that some brines, in some situations, are the perfect solution.
IV.
Here are three candidates for new brines with plausible health benefits:
First, we think there’s evidence that high-potassium brines can cause weight loss.
Ketoade is a term for various concoctions of electrolyte drink, usually high in potassium, that people often drink while on ketogenic diets. People mostly seem to drink this to fight “keto flu”, which may just be the feeling of not having enough electrolytes. But ketoade might also be part of the reason that people lose weight on keto diets. Not from the diet — from the extra potassium.
When we ran the potassium trial, people took supplemental potassium, usually in water or as part of a concoction. On average, people lost weight, a mean of 0.89 lbs over 29 days (n = 104, p = .014).
Despite being statistically different from zero, 0.89 lbs obviously isn’t much in practical terms. But people who took more potassium lost more weight on average (r = -0.276, p = .005), which is additional evidence that there’s something here. And three people lost more than 10 lbs, suggesting that there might be specific ways of taking potassium that are especially effective.
These three participants seem to be more than outliers. For example, here’s one of their reports:
(77174810) First of all – holy shit! It’s amazing how well this worked and it’s also surprising that it’s never really been studied before! Thank you for the analysis and thought that you put into this. For this trial, I basically just ate whatever I felt like, went to a football tailgate party nearly every weekend with lots of beer and foods you would not associate with dieting… and still lost nearly 10 lbs!
…
I have tried every diet/exercise and variation of CICO, atkins, keto, IF, etc., etc., etc. to try and lose weight. To no one’s surprise, nothing really worked for long and the weight always came back. At the end of 2020 I was over 275. It took me three months of busting my ass to lose 20 pounds and as soon as I started eating “normally” again, I slowly started putting weight back on.
Of interest to our point today, this participant took his potassium in solution. If there is an ideal brine for losing weight, it might look something like this:
(77174810) What I discovered was that mixing [potassium] with Simply Strawberry Lemonade makes it very palatable! I dissolved the KCl and a little sea-salt in about 1 oz of water. Then added about 4-6 oz strawberry lemonade. You could damn near sip it this way! Apple cider was the second best mixer.
But the strongest evidence that high-potassium brines can cause weight loss is certainly Krinn.
After some success as a participant in the potassium trial (6 lbs lost), Krinn decided to keep going, increasing her potassium intake and searching for a protocol that she could stick to long-term. At the six month mark, she wrote a tumblr post as a report about her progress. You can read her report here and our review of that report here. Here’s how she describes her approach:
I decided to stabilize at about 10,000mg [potassium] per day … because that’s about how much potassium people were getting during the SMTM potato diet community trial. … Aiming for that amount also meant that it would be easier to compare my results to something that worked decently well and to ask questions like ‘is there something special about whole potatoes, or is it mostly the potassium?’ If it’s mostly the potassium, you’d expect my results to be closer to the full-potato-diet results than to the low-dose-potassium results — which is what happened.
We can also offer a brief update on Krinn’s progress after just over one year (shared with her permission). Take a look at the plot below. As you can see, her weight loss continued until she hit a plateau at just above her target weight, which corresponds to a BMI of 25. She tells us that she’s not sure if this is because the potassium stopped working, or if it’s as a result of external life situation reasons.
Krinn took her potassium as a brine. Specifically, she mixed potassium chloride with Gatorade. Here are the details:
I used potassium chloride powder (whatever came up first on an Amazon search since all KCl should be alike) mixed with regular Gatorade (i.e. not the sugar-free kind) to make it taste okay (I recommend blue Gatorade, it’s the closest to appealing when kaliated — the yellow lemon-lime was meh and the fruit punch red was awful). I added two heaping teaspoons of KCl powder to a 20oz. bottle of Gatorade and drank that. KCl is about 52% potassium and a heaping teaspoon of it is about 6500mg, so I rounded up a smidge and called that 6600-and-a-bit milligrams of potassium per bottle. On Thursdays and Sundays I have drank 2 full bottles and on other days 1.5 bottles. I recorded this as 10,000mg of potassium on regular days and 13,500mg on Thursdays and Sundays.
Comparing Krinn to the participant we mentioned above, who mixed their potassium chloride with strawberry lemonade, we notice a few things in common.
Both of their potassium solutions contained sodium — Krinn from the Gatorade, while the other guy added sea salt. Both of them included sugar, from the Gatorade or the strawberry lemonade. Given what we know about ORS, it seems reasonably plausible that sugar might have an important interaction with potassium. And curiously, both included citric acid, since both Gatorade and strawberry lemonade contain some citric acid.
The biggest difference is the potassium dose — Krinn was getting about 10,000 mg a day from her brine, while the other participant was getting only 3,000 mg/day or so. If there is an ideal weight-loss brine, it probably exists somewhere in the neighborhood of these two approaches.
(That said, it’s not clear that such high doses of potassium are safe for everyone, and they almost certainly are not safe if you have kidney disease or related diseases like diabetes. Do not try supplementing doses this high without consulting your physician, and absolutely do not try it if you have kidney problems or any conditions that might compromise your kidney function.)
In our review of Krinn’s post, we also noted two things. First, Krinn was getting lots of magnesium on the side, through the rest of her diet. And second, she seems to eat a diet high in stearic acid. These are both ingredients that have attracted some suspicion for possibly being related to obesity, which caught our attention. You could plausibly add magnesium to your brine without any trouble (and some brines like LMNT already include a small amount of magnesium). But stearic acid is a butter-like waxy solid, it would probably not go well in most brines, though it is found in milk. Is dairy a weight-loss brine? Well, ExFatLoss would probably say yes..
Our second brine candidate is that we suspect there might be a brine or brines for IBS.
ORS was made to treat the dehydration associated with diarrhea, not the diarrhea itself, but even so it was designed to specially calibrate your digestion. “I’ve had IBS-D,” writes u/feelslikehel, “for about 8 years. I’ve been doing the salt and water regimen for about 6 weeks now and it’s not really making me feel less dizzy but I’m finding that my IBS-D is pretty much gone.” If you have IBS with diarrhea, it might be worth mixing up some ORS. If nothing else, it will help keep you hydrated. Also compare: Large increases in sodium intake are recommended for POTS.
Or how about “Hot girls have IBS”? Hot girls tend to have something else in common — we pay a lot of attention to what we put in our bodies. No processed food, nothing that might disrupt the microbiome. Have you been avoiding salt and sugar to help with your digestion? If so, remember that both sodium and glucose are necessary for your body to absorb water from your gut.
FINALLY
Finally, our third candidate is that there might be a magnesium brine for migraines.
There’s some evidence that oral magnesium supplements can make migraines less intense and less frequent (meta-analysis). This evidence could certainly be more consistent. But as we’ve previously seen, sometimes the right mix can be a big multiplier. Perhaps there is a magnesium brine that would be so much more consistent, or more effective.
But even assuming there does exist some brine that will treat your ailment, or will just help you feel less groggy in the morning, you still need to find it. Or to put it another way, you’d need to discover its location in a high-dimensional brinespace.
IV.
The space of all possible brines is very large. To find other brines with health benefits, we will need to develop new tools.
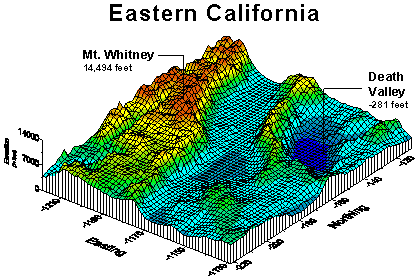
Behold! A 3-dimensional representation of a (hypothetical) high-dimensional brinespace, with height and color indicating “impact on migraines”. The red areas of brinespace are regions of brines that will make your migraines worse; the yellow areas will make no difference; and the blue areas are regions of brines that will make your migraines disappear.
If everyone’s brinespace is largely the same, then it will take only one courageous migrainenaut to map its murky bottoms. But as we know, people are not much the same. And neither are migraines — if there are two or more kinds of migraines, those brinespaces will have to be mapped separately. Perhaps your neighbor’s biology is very different from yours, or she has the other kind of migraine, and her migraine topography looks like this instead:
Who knows what these topologies would look like in real life, how deep their local and global minima might go, how much they might differ between people or over time. But that’s the point. We are going into this with a lot of uncertainty, so we should go into this with caution, and with the right tools.
Disregard, this is Eastern California
Software for searching brinespace should be modular.
❀
The first module would be for the brine ontology, the way of defining the brinespace you want to explore.
Put simply, there are many ways to define a space of possible brines. Some are simple, like the space [mg Na, mg K]. Some are more complicated, like the space [mg Na, mg K, mg Mg, mg Ca, mg Fe, g sugars, mg caffeine].
Some brinespaces make distinctions that others do not. For example, the space [mg Na, mg K, g sugars] treats all sugars as alike, or you could say, treats them as indistinguishable. But [mg Na, mg K, g glucose, g fructose] distinguishes between two common sugars and excludes all others.
Brinespaces can also define their terms in different ways. We’ve been defining these spaces in terms of the mass or volume of the different ingredients (g, mg, L, etc.). But for the scientist mixing brines at home, it might be easier to define these spaces in teaspoons rather than grams, and ingredients like KCl or NaCl instead of the individual elements. This makes it easier to think in terms of making the brine, in terms of operations — how many teaspoons of each ingredient to add to each liter of water.
On the other hand, defining it this way can lead to ambiguous regions of brinespace, and some information may be lost. For example, a brinespace expressed in teaspoons of ingredient salts wouldn’t include the information that adding KCl and NaCl both increase Cl−. If chloride ion concentrations are important, this brinespace would obfuscate that information. With that information, it’s clear that you could add baking soda (NaHCO₃) to a brine to add sodium without any additional chloride ions, or add potassium citrate (K₃C₆H₅O₇) to a brine to add potassium without any additional chloride ions.
Finally, any brine ontology should include some kind of safety limits. A brine might reasonably contain 200 mg/L potassium, but 20,000 mg/L potassium would be dangerous. No need to explore those regions. Exactly where to set these limits is up to the architect, but they should set upper limits on all the dimensions, and set them carefully. Options should be included for special populations, like people with heart conditions, who need to avoid high levels of sodium. Lower limits are not needed — if the dimensions are all at zero, you are simply drinking water. Yum.
Perhaps over time we will find a single large brinespace that is ideal for all purposes. But we might also find that different brinespaces are better for characterizing some searches than others. It’s important that this element be modular, so different brine ontologies can be switched out and tested at ease.
❀
The second module would be the outcome measure. We imagine searching brinespace for mixes that improve health and wellness, and this is the module where we decide how to measure the elements of health and wellness we want to improve.
For example, if you were following Krinn’s example and trying to discover a brine that will help you lose weight, you will want a module that measures your weight loss. A simple measure would be “each brine is rated on how much weight you lose over the next day.” But weight loss can be very noisy, so this might be too sensitive. A better measure might be rating each brine on a weighted average of weight change over the next several days.
If you are looking for something else, you want a different measure. For example, if you have “a horrible grogginess when waking up for most of [your] life” like Romeo Stevens did, you might be looking for a waking-up brine, or a sleepytime brine, to make your mornings a little brighter. In this case you might want a simple measure like, “on a scale from 1-10, how good do you feel 10 minutes after drinking your morning brine?” Or you could do some kind of complicated measure where you test your visual acuity, strength, and reaction time. It’s all the same to us.
If you are trying to find a brine to help your migraines, you could take a simple measure like, “on a scale from 1-7, how bad were your migraines this week?” Or you might find a need for a better scale, like a weighted combination of how many migraines you have each day, and how bad each of them was. You might even include some information about specific symptoms or features.
The point is, there will be many different things that people might want to find a brine for — for weight loss, for their migraines, for after a workout, for general clarity and energy. And for each of these targets, there will be many ways to measure success and progress. Some will be simple, some will be complex, some will just be different. You will want your measures to be modular so people can slot them in and out freely, to reach their own goals as they see fit.
In addition, each module should probably include basic check questions like, “do you like this brine” and “is this brine at all palatable”, as another safety feature. If you find yourself exploring a point in brinespace that you find truly noxious, you should probably just toss that mix and rate it as a failure on all measures.
On the one hand, this approach would exclude potential brines that are disgusting, yet secretly good for you. On the other hand, we doubt that many such brines exist. If a brine is gross, it’s probably bad for you. Your body is in fact designed to deal with these things. And in reverse, if a brine mixture tastes great, that’s an early sign that it might be good for you.
(As a note, you should probably mix your brine with some kind of flavoring. If you drink your brine with water alone, you might accidentally condition yourself to expect that water is dehydrating, something we discovered in the course of our self-experiments.)
❀
Finally, the third module is for the search algorithm and its settings. This is the procedure the software will use for searching the brine ontology or brinespace (the first module you set), and looking for brines that are effective in terms of increasing or decreasing the outcome measure (the second module you set).
Despite the title of this post, the best kind of search algorithm for brinespace is probably simulated annealing. However, we would love to hear elaboration or correction from anyone with more experience in this area.
We shouldn’t assume that the topology of the brinespace will be static for any outcome. In plain language, we might be aiming at a moving target. The best brine today won’t always be the best brine tomorrow. You will be eating other things, exposed to the environment, and also aging. So the search algorithm should always include some amount of exploration, no matter how well it’s doing. It shouldn’t rest on its laurels.
❀
Assuming you define your outcome clearly enough, you choose the right kind of search algorithm, and you give the algorithm enough time, it should eventually find you the best possible brine for your outcome (as measured) within the brinespace you defined.
That’s quite a few assumptions, and assumptions that are easy to get wrong on the first try, or first few tries. If you have spent a lot of time searching with no success, you might want to try different brine ontology modules or different outcome measures, in various combinations. If the software is especially clever, it might be able to help you with this.
But a long search with no success might also mean that there’s no brine that will help with your problem. This is possible and in fact likely in many cases. There is no brine that can cure a broken heart — in fact, high levels of sodium are dangerous for those with heart conditions. But for some problems, the ideal brine or brines may yet be out there.
Special thanks to Krinn and Potassium Participant 77174810 for their pioneering work in the exploration of brinespace.
Krinn is a reader who participated in our Low-Dose Potassium Community Trial. She lost 6 lbs taking low doses of potassium, and liked it enough that she decided to keep going, along with a new exercise habit to help support the weight loss. And she started trying higher doses of potassium, eventually ramping up to around 10,000 mg of potassium a day.
This is a lot — way more than the average person gets from their diet, and a lot more than people added in the original potassium trial.
Krinn writes, “I decided to stabilize at about 10,000mg per day … because that’s about how much potassium people were getting during the SMTM potato diet community trial. … Aiming for that amount also meant that it would be easier to compare my results to something that worked decently well and to ask questions like ‘is there something special about whole potatoes, or is it mostly the potassium?’ If it’s mostly the potassium, you’d expect my results to be closer to the full-potato-diet results than to the low-dose-potassium results — which is what happened.”
Indeed, she lost quite a bit of weight. Here’s the chart of her weight change so far:
Krinn’s report is excellent — nuanced, detailed, and clearly written. She covers almost every aspect of her self-experiment better than we could, so we won’t try to restate her points. We recommend that you read the report for yourself. Instead we will focus on the few small areas where we can add some speculation or additional context.
(Krinn’s full report is also reproduced in an appendix below, because tumblr posts do not always have the best longevity and we figured it might be good for the report to exist in two places.)
Again, you may want to read what Krinn wrote before you take a look at our comments. But we will restate this part: while this seems to be working for Krinn, it’s not clear that high doses of potassium are safe for everyone, and they almost certainly are not safe if you have kidney disease or related diseases like diabetes. Do not try supplementing doses this high without consulting your physician, and absolutely do not try it if you have kidney problems or any conditions that might compromise your kidney function.
Ok, here are our thoughts:
Optimal Weight Loss Brine
Originally, we argued that high doses of potassium alone might be responsible for weight loss on the potato diet. After all, eating nothing but potatoes does give you heroic doses of potassium.
In retrospect, that seems a little naïve. Sure, it could be just the potassium. But biology tends to be a bit more complicated than that.
At risk of oversimplifying (read the original piece), people knew that cholera patients needed electrolytes, but feeding them an electrolyte solution didn’t seem to help.
Through a series of coincidences, people eventually discovered that adding glucose to the electrolyte solution sometimes made the treatment work. But this didn’t immediately lead to a cure, because if you put too much glucose and salt in the solution, it made patients worse instead.
After more confusion, they discovered that sugar and sodium ions are absorbed together in the gut through a sodium-glucose cotransport protein, but you need the right concentration or it will dehydrate the patient instead, which often kills them. The solution was simple, but getting there was hard.
Getting sodium into someone’s body isn’t simple — you need to include glucose in your rehydration formula, and even then, you need to get the right ratios. This makes us suspicious that something similar might be the case for potassium.
Even if high doses of potassium are required for curing obesity, it seems pretty likely that potassium by itself isn’t the whole engine. So now we are looking for some other set of factors, probably other switches that are triggered when you eat ~100% potatoes, that might also be needed to make the gears of weight loss mesh.
Magnesium
The most likely candidate at this point seems to be magnesium.
Potassium and magnesium serve many complementary roles in our biology, and the two minerals are often prescribed together. We spoke to a physician about this, and he pointed out that for patients with low potassium (hypoK), if you don’t have enough magnesium (hypoMg), you’ll be hypoK forever unless you fix the hypoMg first, because of “some renal excretion thing I think” (his words). See also this paper, which says: “magnesium replacement is often necessary before hypokalemia and potassium depletion can be satisfactorily corrected with potassium supplements.”
Electrolyte mixes, like LMNT and Snake Juice, are sometimes used for weight loss, and these mixes usually contain some amount of magnesium. Assuming that, by a process of natural selection (it’s a electrolyte-powder-eat-electrolyte-powder world out there), they have run across something like the right electrolyte ratios to cause weight loss, this also suggests that magnesium might be involved.
Like potassium, most people are not getting enough magnesium, at least per the official recommendations. According to the NIH, you’re supposed to get 300-400 mg of magnesium per day. And potatoes are not only high in potassium, they are also pretty high in magnesium. Each potato contains about 40-50 mg of magnesium. Someone on the potato diet would be getting about 800-1,000 mg of magnesium per day.
If potassium and magnesium together are the cause of this weight-loss effect we’ve discovered, this would explain why potatoes are such a reliable way to cause weight loss, and why they’re often more effective than supplementing straight potassium.
All the above are just reasons for the hunch, but we also want to note that this hunch is supported by Krinn’s case study.
In her report, Krinn writes:
My go-to snacks are cashews, pistachios, cherries, and granola bars.
Cashews and pistachios are particularly high in magnesium, providing 260 mg per 100 g and 110 mg per 100 g, respectively. We don’t know exactly how much cashew Krinn is consuming, but it’s likely that it’s giving her a respectable amount of extra magnesium.
We discussed this with Krinn over twitter DMs, where she said, “cashews are one of my go-to snack foods, so whatever amount I’m getting, I would be extremely surprised if I was getting something less than a healthy amount of magnesium in my diet.”
She also notes that she tends to consume the magnesium and the potassium relatively close to one another.
…another way to look at it is that “eating cashews” and “drinking gatorade+potassium” are never _that_ far apart
since the potassium stuff is spaced out 4–6 hours apart across the day, and I eat cashews at least once a day, that puts a ceiling on how far apart those two things could possibly be
We have no idea if it’s helpful or necessary to take potassium and magnesium at the same time, but it’s worth noting that Krinn tends to leave little daylight between them.
In short, we’ve suspected for a while that potassium might only cause weight loss, or might cause it more effectively, when combined with reasonable doses of magnesium. The potato diet would get this “for free”, since potatoes contain high amounts of both. This hunch predicts that people who lose weight by supplementing straight potassium will also likely be getting high doses of magnesium from some source, either from supplements or their diet. Krinn’s case matches that prediction.
We’ve also recently been corresponding with a participant from the half-tato diet, who told us that straight potassium seems to have some kind of effect for her, and who mentioned that she has been supplementing 266 mg magnesium a day as magnesium glycinate capsules. Not conclusive, but another hit for the prediction.
Stearic Acid
Another possible connection is with stearic acid, a fatty acid found in “meat, poultry, fish, eggs, dairy products, and foods prepared with fats; beef tallow, lard, butterfat, cocoa butter, and shea butter are rich fat sources of stearic acid.”
If you’ve heard of this before, it’s likely from Fire in a Bottle (FIAB), a website/program/theory which argues that a diet high in stearic acid can cause weight loss. This is sometimes called The Croissant Diet (TCD), presumably in the hopes of confusing readers — you do not actually eat nothing but croissants. In fact, you don’t have to eat any croissants at all. But you do ideally eat lots of foods high in stearic acid, sometimes supplementing with additional stearic acid, and some people seem to lose weight when they do this.
We find the evidence for stearic acid to be pretty thin (though see FIAB for the other side). And there’s no theoretical reason to suspect that stearic acid influences potassium uptake or anything. But there are just a few hints, so we figured we might mention them here.
One is from our half-tato diet. Most people lost only a small amount of weight on the half-tato diet, but one person (participant 25348806) lost 17 lbs in four weeks. This person gave us detailed notes about the rest of her diet, and this part jumped out in particular:
…I also have dairy – at least one glass of milk a day (either raw whole milk or 2% or whole conventional) – and a small amount of juice or lemonade. Some mornings I may have full fat yogurt with collagen and stearic acid (see fireinabottle.net) but not all mornings. I have some extra potassium as well as other supplements.
For comparison, here’s what Krinn has to say about her fat intake:
I use a generous hand when measuring out olive oil. I believe that if you need either milk taste or milk fat, you shouldn’t half-ass it, so when I need milk taste or milk fat, I rely on whole milk and heavy cream. Fats, generally, taste good. … Once in a while, dark chocolate, usually with the nuts and fruit.
Milk fat and chocolate (via cocoa butter) are both high in stearic acid. You’ll also notice that Krinn usually takes the chocolate with her cashews.
And remember that participant from the half-tato diet we mentioned at the end of last section? Based on these hints, we asked her if she also consumes a lot of stearic acid, and she told us she eats a whole lot of dairy fat, and chocolate “EVERY DAY” (her emphasis).
This is certainly suggestive, but what doesn’t fit is the potato diet. Potatoes are high in both potassium and magnesium, so it would make sense if high doses of potassium and magnesium conspire to create the potato weight loss effect. But potatoes contain very little fat and approximately 0% stearic acid. The idea that you might need stearic acid to cause the potato effect is rather inconsistent with the potato diet, since you do not get appreciable amounts of stearic acid from potatoes.
That said, there are hints that people who are on half-tato, or who are supplementing potassium directly, do benefit from stearic acid. At the very least, we’ve noticed that some of the biggest success stories are people who have been getting decent amounts of stearic acid in their diet. Maybe stearic acid helps when you are getting less enormous doses of these minerals?
It’s always possible there’s some unknown connection — maybe the potato diet only works for people who already have sufficient reserves of stearic acid in their body. Or maybe some people need stearic acid for the effect to kick in and others don’t, for genetic reasons. Or maybe other fatty acids can substitute in a pinch, but stearic acid happens to be slightly better than average. But at this point, it definitely fits less well than magnesium.
This Age Needs Heroes
We love everything that Krinn did here. She participated in a community trial, decided to keep going, and spun it into a self-experiment. She came up with her own design and attacked her questions in her own unique way. She did something interesting and she wrote it down so that all ingenious people could be informed thereof and consider the results for themselves.
More people should do what Krinn did, and get involved in the business of conducting science. Anyone else who wants to do anything else remotely like this should feel free to reach out, we’d be happy to help. We’re in the process of writing a whole series about how to conduct self-experiments, which may be a good starting point. Consider this your invitation.
Here’s a reproduction of Krinn’s full report as it appears in her tumblr post:
An Ad-Hoc, Informally-Specified, Bug-Ridden, Single-Subject Study Of Weight Loss Via Potassium Supplementation And Exercise Without Dieting
Here’s the short version: I lost 30 pounds in 6 months by chugging a bunch of potassium salt and exercising a lot. My subjective experience is that cranking my potassium intake way up made it possible to do a lot more exercise than I had been doing without also eating a lot more. Exercising more without also eating more led to weight loss (as one would hope!). I did not diet: I ate as I had been doing and as it pleased me to do. Do with the raw data as you please.
Losing weight this way is unusual and worth paying attention to because many things about increases and decreases in weight and obesity are very poorly understood. Many people would like their personal weight and obesity levels to be different, so anything that improves our collective understanding of how to make that happen is valuable. However, losing weight this way is an experiment: it’s not necessarily safe to do what I did! Part of why I did it was to find out what would happen, and if you have any kind of existing kidney problems then you definitely should not do what I did. Note to other transfemmes: if you’re taking spiro, that counts as a kidney problem.
I also don’t want to overstate the significance of this experiment: what I’ve been up to in the last 6 months amounts to a single data point that happens to also be 1,100 spreadsheet cells. It’s a data point that is highly suggestive, sure, but it would be extremely ambitious to say that it proves anything beyond “this worked for me” and perhaps “it’s not impossible for this to work”. I am writing about it because as far as I know, this particular experiment is something that nobody else has tried, and, again, anything that improves our collective understanding here is valuable.
The long version comes next: how I came to be doing this experiment, what I did in the experiment, what I plan to do next, and finally what I think about it all. The really long version is the ongoing conversation that this post is part of, starting with A Chemical Hunger, which is a book-length literature review about the 1980s–present global increase in obesity prevalence, also the posts about single-subject research where the same authors discuss the limits of what can be learned from experiences like mine, also the Experimental Fat Loss guy and his wide variety of diet-only experiments, also somecritics who disagree.
How I came to be doing this
At the tail end of 2022, I noticed both that my BMI had hit 30 and that I had become very unhappy about my weight. There’s a specific photo where I didn’t realize until I saw the photo that my belly was hanging out over my waistband and it’s vividly unpleasant in my memory. Around the same time, I happened to find the potassium-supplementation community trial that the Slime Mold Time Mold folks were running. The value proposition was “this will be easy, cheap, and safe, but also it might not actually work,” and that sounded good to me, so I signed up for it and took a modest amount of potassium all through December and January. It kinda-sorta worked: I lost 6 pounds. Not nothing, but “it kinda-sorta worked” is the most one can really say about losing 6 pounds in 60 days.
The low-dose potassium delivered on all of what the SMTM folks promised, though. It was easy, cheap, and safe. So I kept doing it and, since I was already doing the potassium, decided that I should get an exercise habit going. I am a big believer in the idea that it’s a tremendous amount easier to go from doing Something to doing More Something than to go from doing Nothing to doing Something. The low-dose potassium got me through the first step: once I was doing Something about my weight, it was relatively easy to do More Something. When the community trial ended in early February, I didn’t have to worry about messing up its results by departing from the trial’s instructions, so I started taking more potassium and building my own experiment. I also kept in touch with the SMTM authors, who were very encouraging. 🐯💕
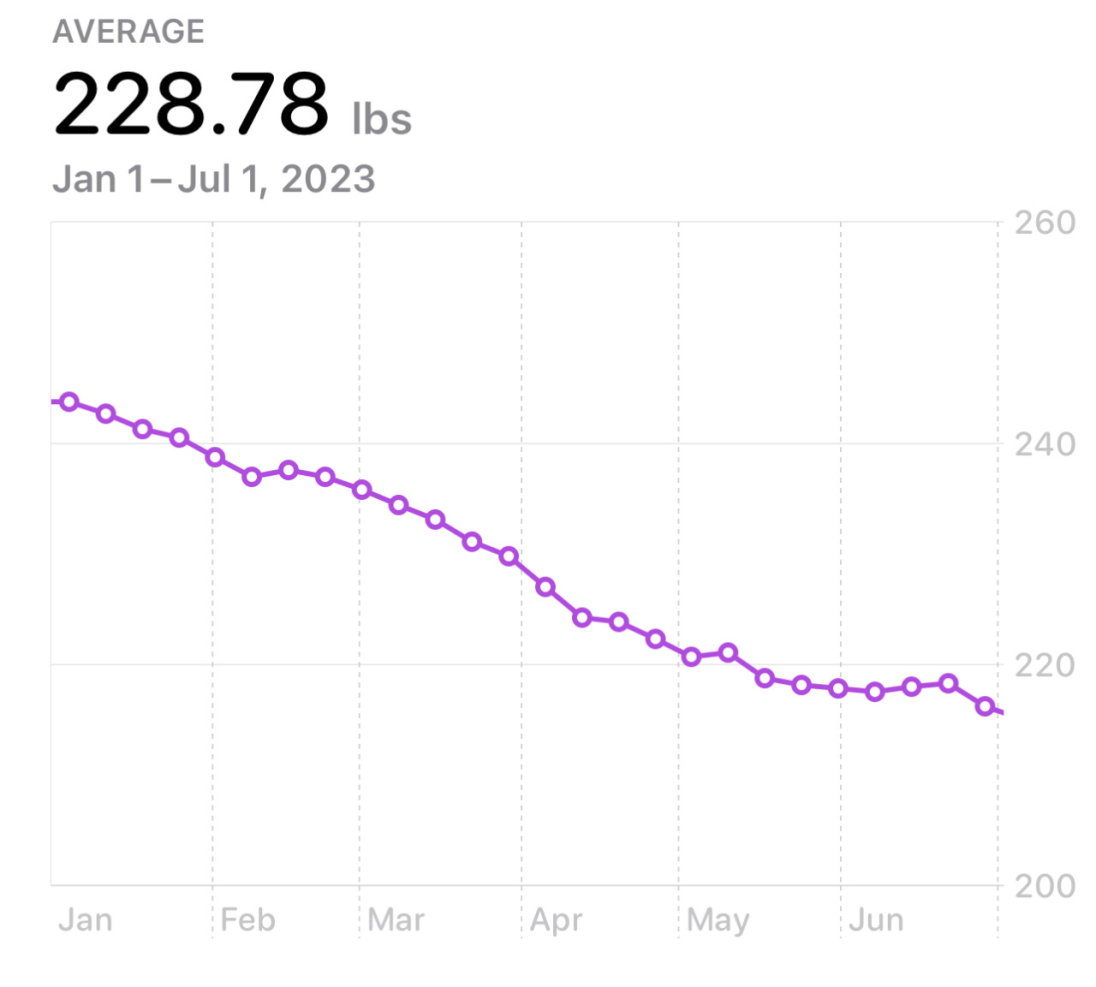
By late March I had brought myself up to daily amounts of potassium and exertion that seemed good to me, and I stuck with those. This is the first time in my life I’ve focused on trying to lose weight, and I was not fully prepared for how demoralizing it is that the weight change from day N to day N+1 sometimes seems perversely unrelated to what you were doing on day N. Fortunately I have experience with spreadsheets, so I put together a tracker for myself that focused on the trailing-week average of my daily weight and exercise measurements as well as long-term graphs. Three months of data were enough to put together a chart whose trendline said very, very clearly, “what you are doing is working — keep it up!” With any kind of long-term project it’s very important to create and sustain sources of feedback. All else being equal, the longer it takes before you can get a read on “is this going well or poorly?”, the worse it will go.
I decided that my goal would be to get my BMI from 30 (the lower limit of “obese”) to under 25 (the upper limit of “normal”). Happily, the math is very easy there: for my height, a BMI of 25 rounds off to 200lbs. I further decided that I was willing to spend all of 2023 working on this. That decision is why I’m writing this post now: halfway through a project is a natural time to pause and take stock.
What I did
By the end of March, my regimen was firmly settled and I kept at it through the end of June without further tinkering. The daily goals I settled on were 10,000mg of potassium and 1,200kcal of exertion. That amount of exercise worked out to be 90 to 100 minutes per day. For contrast, in 2022 my average amount of exercise per day was 15 minutes and my average exertion was 500kcal.
I used my smartwatch’s exertion number (“how many calories are you using above the amount you need to burn to be alive at all?”) and gradually walked up my daily goal, settling at 1,200kcal/day partially because it was working and partially because one hour of watch face equaling 100kcal was helpful for being able to read “how close to my goal am I?” without thinking hard about it. Most of the exercise was treadmill time, usually a brisk walk or light jog. Over the months I also did some running, some bicycling, and some hiking, but treadmill time was the reliable, unremarkable, do-this-every-day core of my exercise regimen. It took a while to ramp up to that amount of exertion and there were definitely days when I stumbled, for good reasons and bad. However, in general I hit the exertion goal and in particular had it absolutely dialed from early March to mid-April.
It was easier to be totally rigorous about the potassium-intake goal — it helped that that part only took a few minutes per day, instead of 90+ minutes! I used potassium chloride powder (whatever came up first on an Amazon search since all KCl should be alike) mixed with regular Gatorade (i.e. not the sugar-free kind) to make it taste okay (I recommend blue Gatorade, it’s the closest to appealing when kaliated — the yellow lemon-lime was meh and the fruit punch red was awful). I added two heaping teaspoons of KCl powder to a 20oz. bottle of Gatorade and drank that. KCl is about 52% potassium and a heaping teaspoon of it is about 6500mg, so I rounded up a smidge and called that 6600-and-a-bit milligrams of potassium per bottle. On Thursdays and Sundays I drank 2 full bottles and on other days 1.5 bottles. I recorded this as 10,000mg of potassium on regular days and 13,500mg on Thursdays and Sundays.
Is 10,000mg of potassium a lot? It’s a lot more than average! The SMTM potassium trial post contextualizes it helpfully:
For a long time, the recommended daily value for adults (technically, the “Adequate Intake”) was 4,700 mg of potassium per day. But most people don’t get anywhere near this amount.
In every CDC NHANES dataset from 1999 to 2018, median potassium intake hovers around 2,400 mg/day, and mean intake around 2,600 mg/day. In this report from 2004, the National Academy of Medicine found that “most American women … consume no more than half of the recommended amount of potassium, and men’s intake is only moderately higher.” Per this paper, only 0.3% of American women were getting the recommended amount. Similarly low levels of intake are also observed in Europe, Mexico, China, etc.
But in 2019, the National Academies of Sciences, Engineering, and Medicine changed the recommended / adequate intake to 2,600 mg/day for women and 3,400 mg/day for men. They say that the change is “due, in part, to the expansion of the DRI model in which consideration of chronic disease risk reduction was separate from consideration of adequacy,” but we can’t help but wonder if they changed it because it was embarrassing to have less than 5% of the population getting the recommended amount.
In any case, recommended potassium intake is something like 2,500 to 5,000 mg per day for adults, and many people don’t get enough.
Potatoes are exceptionally high in potassium. A single potato contains somewhere between 600 and 1000 mg of potassium, depending on which source you look at. They are the 6th highest in potassium on this list of high-potassium foods from the NIH, and 9th on this old list from the USDA. If you do the math, this means that someone on the potato diet, eating 2,000 kcal of potatoes a day, gets at least 11,000 mg of potassium per day, more than twice the old recommended intake.
This explanation is most of why I decided to stabilize at about 10,000mg per day: because that’s about how much potassium people were getting during the SMTM potato diet community trial. Because that community trial involved around 200 people, it was unlikely that there would be any truly heinous health effects from knocking back that much potassium, especially together with the anecdotal evidence that inspired the trial. Aiming for that amount also meant that it would be easier to compare my results to something that worked decently well and to ask questions like “is there something special about whole potatoes, or is it mostly the potassium?” If it’s mostly the potassium, you’d expect my results to be closer to the full-potato-diet results than to the low-dose-potassium results — which is what happened.
I measured those results in a very basic way: ordinary bathroom scale, first thing in the morning, every day. Considering how much noise there is in weight measurement, there’s just no advantage to measuring it more often. I kept the circumstances of the weigh-in simple and stable, trusting that that was good enough. I also measured exertion in two other forms — step count and exercise minutes — but that was mostly for my personal curiosity because both are basically downstream of exertion as such. Similarly, I tracked my sleep but didn’t expect that to matter a whole lot.
While I was affirmatively not dieting, I want to make sure to talk about my food habits because I could be missing something that’s easy for others to see as unusual but seems totally ordinary to me. My meals are heavy on pasta, rice, bread, and granola. I work diligently to get enough dietary fiber. I eat some meat but not a lot (eating a pound of meat in a week would be above average for me), and I enjoy coffee but not a tremendous amount of it since usually I make Chemex-style coffee and having a bunch of that in a day would be too time-intensive. My go-to snacks are cashews, pistachios, cherries, and granola bars. Like most people, I should eat more dark leafy greens than I do. I use a generous hand when measuring out olive oil. I believe that if you need either milk taste or milk fat, you shouldn’t half-ass it, so when I need milk taste or milk fat, I rely on whole milk and heavy cream. Fats, generally, taste good. I eat more whole food and food I personally cook than I eat packaged and processed food, and I only infrequently eat restaurant food (weekly pizza night, maybe twice a month other than that). I really like sour candies but basically stopped eating them last autumn after some very patient coaxing from my dentist. Once in a while, dark chocolate, usually with the nuts and fruit.
I ate as I had been doing: I ate the food I felt like eating and ate as much of it as I felt like eating. If I felt like eating more or less, I did that. Since I wanted to keep the exercise habit going regardless of whether or not I lost weight, it was very important to me to not make the exercise any more difficult than it had to be. Going hungry would definitely make it more difficult, so I avoided doing that. One way in which I’m very sure my experience generalizes is, it’s much easier to persuade people to try “add this supplement to what you’re already eating” than to get them to try “replace all of your current food with potatoes,” especially when talking about long-term or indefinite-duration changes.
What I plan to do next
I’ll be thrilled if I can recapture something like the 7-week March/April streak I had going. Most days in this period (44 out of 49) were PB days (i.e. a day where my trailing-week-average weight was the lowest it had been since the start of the year) and no two consecutive days in this period were non-PB days (i.e. if a day wasn’t a PB day, both the day before and the day after were PB days). I was losing almost 2lbs per week and exercising a lot and I felt great. However, my intuition is that that was the honeymoon period of going from mostly-sedentary to exercising regularly, and that I should expect further progress to be more difficult, to be like the less impressive results I got in May and June.
Still, the thing as a whole has definitely been successful enough that I’m going to keep at it until the end of the year, re-evaluating again in December (and maybe when I hit my weight-loss goal, which should happen around halfway between now and then). Since I’m using January 1st as my anchor date for the start of the experiment, it lines up nicely with the calendar if I just keep going all year and see what happens. Besides, I only need 6 months more to generate a year of data, while someone going from a cold start would need a whole year.
Given that I have a setup that is working pretty well, I’m reluctant to tinker with it. I might add one more high-potassium day in addition to Thursdays and Sundays, and I might start tracking some extra data — even though I’m not trying to change them, recording my food habits seems like the most helpful additional thing I could record.
If I develop health problems I’m gonna pull the ripcord (and post about it). There are already too many shitty fake weight loss regimens in the world that fuck up the health of people who try them, we do not need more.
What I think about it
Since I’m the one doing this experiment, I get to be excited about how it’s working out for me personally, which is to say, very well indeed. Right now it seems pretty certain that I’ll be able to reach my goal of losing ~50lbs in a long-term-sustainable way and just as importantly, getting myself to a much better baseline state of physical fitness. I feel pretty great about that part!
The experiment is not just for me, though: the reason it’s an experiment rather than just “I’m trying to lose weight” is that I am keeping track of things carefully such that other people could carry out the same steps I did and get results similar to or different from mine and ideally everyone eventually comes to pretty firm conclusions about whether this — losing weight via potassium and exercise without dieting — works or not. My chugging potassium and Gatorade for six months to a year is the very beginning of that process, and I expect that the difficult parts of the process will be carried out by people with more expertise and resources than me.
I also expect that I have not tumbled to the One Weird Trick for weight loss that everyone else just overlooked. As someone with plenty of programming experience, I have a hearty suspicion towards “well, it worked on MY setup” stories. One obvious alternate explanation for my successful weight loss is “well yeah, you doubled your exertion and kept your food intake the same, of course you lost weight” — but I don’t find that explanation satisfying. To start with, if it were that easy, people would do it more often. There are a tremendous number of people who would like to lose weight and a tremendous marketplace of devices, services, and professionals to help them use exercise for that purpose, and yet in a 20-year NCHS study, average exercise rose without obesity falling. It’s also very, very easy to find fat people who exercise plenty — you will find them more or less anywhere you find lots of people exercising, as well as in places like sumo stables. A member of my family has taken up powerlifting in the last year, making him both fitter and heavier by quite a bit.
Additionally, there’s studies like Keating 2017 concluding that short-term exercise intervention doesn’t do enough to matter, or like the Wu 2009 work concluding that exerise-and-dieting isn’t meaningfully better than just dieting over periods of 6+ months, and then there’s the STRRIDE study, Slentz 2004, concluding that jogging 20 miles a week can get people to lose about 7 pounds over 8 months. The STRRIDE study caught my eye because it’s pretty similar to what I did: they took obese mostly-sedentary folks, had them exercise more, and forbade them from eating less. However, once you do the math the results are much less similar: the average STRRIDE participant did around half the exercise I’ve done for at most a fifth of the weight loss (i.e. around 1lb/month vs. around 5lbs/month and around 3mi/day vs. 7mi/day). If someone else told me “Krinn, your naïve just-hit-the-treadmill exercise regimen is 2.5x as effective as an exercise regimen supervised & measured by professionals,” I would want them to provide some compelling evidence for that.
If you tell someone you want to lose weight and would like their advice, it is overwhelmingly likely that the advice will involve exercising more. Everyone has heard this advice. And yet, as Michael Hobbes observes in a searing piece for Highline, “many ‘failed’ obesity interventions are successful eat-healthier-and-exercise-more interventions” that simply didn’t result in weight loss. Even if we as a society choose to believe “more exercise always leads to weight loss, most people just fuck up at it,” that immediately confronts us with the important question, why do they fuck up at it? and its equally urgent sibling, what can we learn from those who succeed at it to give a hand up to those who have not yet succeeded?
[exercising more and eating less] is not an explanation any more than “the bullet” is a good explanation for “who killed the mayor?” Something about the potato diet lowered people’s lipostat set point, which reduced their appetite, which yes made them eat fewer calories, which was part of what led them to lose weight. Yes, “fewer kcal/day” is somewhere in the causal chain. No, it is not an explanation.
Since I’ve been doing this for six months, I feel pretty certain that the potassium is doing something positive for me and I’m entirely willing to put in another six months to find out what happens for me. Finding out whether that generalizes is beyond my power: all I can do is explain what worked for me, one middle-aged Seattle housewife, and hope that it’s useful to people who are in a position to do serious work about it.
One kind of serious work that’s available is the very cool analytic techniques that other people in this conversation have used while looking at their data. If you are the kind of person to get elbows-deep in R or Matlab, feel free to grab my day-by-day measurements for that (I release this data under Creative Commons’ CC0 if that’s relevant to you). I’m not going to do that, though, partially because it’s been a long time since I last used R but mostly because of the thing I said earlier about my whole experiment basically being one data point. If you have a data series, then yeah, get in there with some numeric interrogation, but if you only have one data point, that data point is what it is and statistical analysis can’t really add to it. All I can claim here is that this is a new data point: people going about their everyday lives do not spontaneously increase their potassium intake severalfold and the background work from the SMTM potato diet and potassium community trials tell me that no-one’s run a study looking directly at what happens if you do increase your potassium intake that much.
Do you want to increase your potassium intake that much? If you do, I have to re-emphasize the potassium community trial‘s safety warning: if you have existing kidney problems, do not try this. Also I’m gonna deploy the boldface again to make sure I get this across to other trans women: on this topic, taking spiro counts as a kidney problem! I am not a doctor and I’m extremely not your doctor, you should talk to your actual doctor if you have any kind of potential kidney issues and even if you’re in good health and want to try chugging a bunch of potassium, you should titrate up gradually the way the SMTM writeup suggests (which is also the way I did).
In addition to a general spirit of responsibility, those warnings are important because otherwise just telling you that this is easy would sound like a recommendation. Did I mention that the experiment was easy? Easy easy. Piss easy. Lemon squeezy, etc. Of course building an exercise habit wasn’t easy, but the potassium part didn’t make it easier or harder, and the potassium part itself was pretty trivial. Mix this powder into Gatorade a couple times per day, drink it, done.
That said, if you do want to try this, godspeed and please write down how it goes for you. I recommend building positive reinforcement into whatever you use to track it; my personal spreadsheet for this is adorned with color-coding and happy emoji. I also recommend at least thinking about the following questions, whether you’re going to do this, evaluate the results of this, or both.
How safe is it, in general rather than for me particularly, to chug this much potassium? This is the big one: “just mix potassium salt into Gatorade and drink it a few times a day” is so incredibly easy that even if the effect size is small, it could benefit a huge number of people, but of course it doesn’t benefit them if it’s not actually safe to do that.
Does this replicate? If it’s not safe it matters a lot less whether it replicates, so the safety question comes first, but if it is safe, then one would immediately want to find out whether it works for 1% of people, 10% of people, or 50% of people.
How much do other mineral nutrients, particularly sodium and magnesium, matter for this? Maybe they need to be combined in some specific way, as this Twitter thread suggests.
Do sex hormone levels matter? I’m a trans woman and I’ve been having problems with access to HRT in this timeframe. Given how many things in one’s body testosterone and estrogen affect, and given that previous obesity research has shown differences based on hormone profiles, that’s definitely something to keep an eye on. Also because spironolactone in particular messes with renal function and potassium metabolism, I expect that it affects this. Digression: spironolactone is total bullshit as an anti-androgen of first resort. It sucks and I hate it and I should have switched to other anti-androgens even sooner than I did. If you’re using spironolactone as an anti-androgen because it was the first thing your doctor tried for that, you really should try something else and see if that works.
I steadfastly avoided dieting. I like my existing diet just fine, and that’s why I preferred the “what if I just chug a bunch of potassium” plan. All else being equal, I’d rather try things that let me eat what I like than things that require throwing my relationship with food into upheaval. But of course you wonder, what would happen if you did combine dieting and exercise and potassium? The ExFatLoss guy has been busy trying a lot of diet-only interventions and he’s got a lot of interesting results. I am not the person to try it, but it’s one of the obvious things to try, so I hope someone does try it.
How does this interact with the munchies? If you decide to try what I tried and you, like me, enjoy living somewhere where marijuana is legal, I think you should look at whether the potassium changes how you experience marijuana-induced hunger/overeating. One of the things I found very striking about the matter is that it was possible for me to chug enough potassium that the marijuana-induced hunger was drastically reduced. I expected the opposite since the potassium was causing me to eat less (relative to exertion) at other times. However, I have very strong habits about marijuana (exactly twice a week, edibles only, same amount every time) and I’m not willing to change them for this, so who knows how this aspect will work out for others. Definitely something to keep an eye on, though. Even if I wasn’t losing weight, the potassium reduces marijuana-induced overeating enough that I’d probably keep going with it just for that effect.
Conclusion
I spent 6 months trying to lose weight with lots of potassium and exercise but without dieting. So far I have succeeded. Unless something disastrous comes up, I’m going to keep trying it for at least another 6 months and going to keep recording what I’m doing. I’m particularly curious to see where I’ll plateau, since I assume at some point I’ll start getting really hungry and/or tired instead of accidentally starving. I hope that my experience and the data I’ve recorded from it, are useful to people who are looking into questions about obesity and weight. Please feel free to use my data and my writeup (this post) for that. If you want to try doing as I’ve done, good luck and stay safe: this has worked for me but it is still experimental, it might be unsafe and/or fail to work for you.